
Premenopausal: Very Low E2 + Progesterone
Disclaimer
The Fullscript Medical Advisory Team has developed or collected these protocols from practitioners and supplier partners to help health care practitioners make decisions when building treatment plans. By adding this protocol to your Fullscript template library, you understand and accept that the recommendations in the protocol are for initial guidance and may not be appropriate for every patient.
Protocol: Very Low E2 + Progesterone <2ng/mL (A/B)
General Protocol (no or low symptoms):
- Vitamin B6
- Vitex Agnus Castus Extract
- Vitamin A
- Vitamin E
Further considerations:
E2 results within or below the postmenopausal range may imply ovarian failure. Test LH + FSH (blood).
Additional Protocol (low symptoms):
- Consider phytoestrogens:
- Black Cohosh Extract
- Dong Quai Extract
- Genistein
- Daidzein
- Red Clover Extract
Note: the products selected for the protocol are based on the above ingredients and the most commonly recommended by practitioners in the Fullscript community.
Lab Assessments: Progesterone | Estrogen
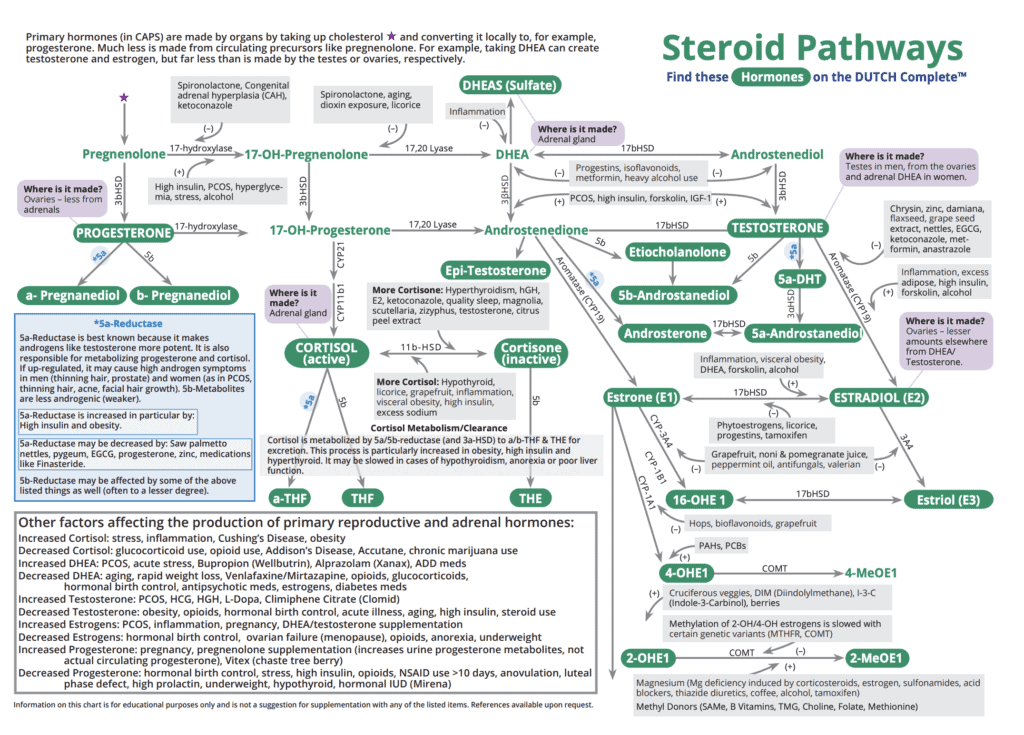
Assessing Estrogen Status:
Estrogen status (low, normal, or high) is primarily based on the hormone estradiol (E2). Postmenopausal women make about 10 times less estrogen, mostly of adrenal origin. While E2 is the strongest estrogen, estrone (E1) and 16-OH-E1 are also significantly estrogenic. Carefully consider all estrogen metabolites, but give more weight to the levels of E2.
“Optimal” levels may depend on many factors, including the corresponding Pg values and patient history and symptoms. This guide may not be appropriate for women on HRT and the categorizations are made assuming women are NOT on HRT.
Assessing Estrogen Metabolites:
Estrogen metabolites must also be considered. E1 and E2 are both metabolized by three competing (2, 4, and 16-OH) pathways. Generally, metabolism that heavily favors 4-OH is considered a potential risk factor for estrogen-related cancers (although this is a complicated issue). Conversely, 2-OH metabolites (particularly 2-methoxy estrogens) are considered more protective.
“Poor Phase 1 Metabolism” on page 11 and 12 generally refers to a pattern that favors 4-OH or 16-OH estrogens over the more protective 2-OH estrogens. “Poor Methylation” refers to a patient who is not readily converting “hydroxy estrogens” (like 2-OH-E1) to “methylated estrogens” (2-methoxy-E1). Both of these patterns can be assessed on the estrogen metabolism page of the DUTCH test.
*Some scenarios on this guide may suggest Hormone Replacement Therapy (HRT). All HRT may have risks which must be understood by a provider before considering any HRT.
Assessing Progesterone Status:
Progesterone (Pg) is categorized into four groups for women:
- 0-0.5ng/mL – The adrenal glands make most of the Pg after the ovaries quit. If levels are very low, adrenal and ovarian hormone product of Pg may both be low.
- 0.5-2.0ng/mL – The normal range for a woman who is not cycling/ovulating and has proper adrenal Pg production.
- 2.0-6.0ng/mL – Most likely represents one of the following scenarios: A) A woman who has ovulated but makes insufficient Pg for a premenopausal woman. B) A postmenopausal or anovulatory woman whose adrenal production of Pg is slightly higher than normal.
- >6.0ng/mL – Women with levels above 6.0ng/mL have likely recently ovulated. We consider >12.0ng/mL to be strong Pg production.
Note: The Pg assessment is based off of two urine metabolites (a – Pregnanediol and b – Pregnanediol) that are extrapolated to provide an individual “serum equivalent” number that has been shown to correlate to serum Pg measurements.
Disclaimer
The Fullscript Integrative Medical Advisory team has developed or collected these protocols from practitioners and supplier partners to help health care practitioners make decisions when building treatment plans. By adding this protocol to your Fullscript template library, you understand and accept that the recommendations in the protocol are for initial guidance and may not be appropriate for every patient.
Disclaimer
The Fullscript Medical Advisory Team has developed or collected these protocols from practitioners and supplier partners to help health care practitioners make decisions when building treatment plans. By adding this protocol to your Fullscript template library, you understand and accept that the recommendations in the protocol are for initial guidance and may not be appropriate for every patient.