Elevated Serum Vitamin B12: Causes, Workup, and Clinical Meaning


A patient comes in after routine blood work, and the report flags a serum vitamin B12 of 1,250 pg/mL. No one ordered the test to find a high value. It was meant to rule out deficiency, but the result points the other direction. Often the explanation is simple and benign, often iatrogenic, meaning it comes from B12 the patient is taking or being given. Sometimes it can be an early clue to a hepatic, renal, hematologic, inflammatory, or malignant process. Sometimes it is an artifact of the assay itself.
An elevated serum vitamin B12 is easy to misread, because the test was built primarily to detect the opposite problem. The number reflects the binding proteins the assay measures, the platform that produced it, what the patient has been exposed to, and the clinical picture around it. This article outlines an approach to interpreting and working up a high serum B12 in adults by separating four possibilities: intake-related elevation, disease-associated hypercobalaminemia (an elevated blood B12 associated with an underlying condition), analytical interference, and functional deficiency.

Sleek consumer lab tests offer data, not direction
Influencer-driven lab companies with AI doctors? That’s not how real health functions. Fullscript Journeys gives you the easy lab testing experience you want and a provider to support you when the real work begins.
What an elevated serum B12 represents, and why no single threshold exists
A serum B12 reflects vitamin bound to transport proteins in the blood, not the amount that has reached the tissues, and the threshold for calling it high shifts with the assay, the laboratory, reference interval, and the unit on the report.
Cobalamin transport physiology behind a high result
Two proteins carry vitamin B12 through the blood. Haptocorrin, also called transcobalamin I, holds roughly four-fifths of the circulating vitamin, and transcobalamin carries the rest. The transcobalamin-bound fraction, known as holotranscobalamin or active B12, accounts for 6%-20% of bound vitamin B12. (4)
Most of what a total B12 assay measures is bound to haptocorrin and is not available for uptake by most cells. Holotranscobalamin and the metabolic markers generally track what is happening inside the tissues more closely than total B12 does. (6)
The liver and kidneys shape the number further. The liver stores cobalamin and clears the haptocorrin-bound form, releasing the vitamin into bile. The kidneys clear B12 as well, and any free vitamin that exceeds the binding capacity of these proteins is excreted in the urine. (4) When either organ slows down, B12 can accumulate for reasons that have nothing to do with intake or tissue need.
Reference ranges, units, and the absence of a universal upper limit
There is no single number that defines a high B12. In healthy adults the total concentration sits around 200 to 600 pmol/L, but the upper reference limit varies by laboratory and by analytical platform. (4) Studies of unexplained elevation have used cutoffs that do not even agree on units. Some define elevation as a value at or above 1,000 ng/L, which is the same as 1,000 pg/mL and roughly 738 pmol/L, while others set the bar at more than 1,000 pmol/L, closer to 1,355 pg/mL.
The unit on the report changes how the number should be read. A result of 1,000 reads very differently in pg/mL than in pmol/L, so whether a value counts as high depends on the unit and the laboratory reference interval.
Vitamin B12 has no tolerable upper intake level, because its potential for toxicity was judged too low to set one. (9) That refers to oral intake, not to the blood level. A high serum value can still carry clinical meaning even though there is no established upper intake limit for oral B12.
Some laboratories report may show a very high result as greater than a stated upper limit rather than as a precise number. (4) If the exact value would change management, the clinician may need to ask whether dilution or another confirmatory step is available, since "greater than 1,000 ng/L" can hide a B12 level that is markedly elevated.
Reading the result as a marker, not a diagnosis
A high B12 indicates a cause to be identified rather than a diagnosis on its own. It can mean more binding protein in circulation, vitamin released from injured cells, reduced clearance by the liver or kidneys, recent intake, or analytical interference, where the measured value does not accurately reflect the true B12 status. (4) Each explanation leads to a different follow-up question.
Persistent elevation carries a far stronger association with serious underlying disease than a transient one. (7) A single elevated reading after a supplement or an injection rarely means the same thing as a value that is still elevated on a repeat test weeks later.
What a high B12 means depends on the rest of the picture: the timing of the last oral or injected dose, the patient's symptoms, the examination, and the other laboratory results.
Intake-related elevation as the most common explanation
Most of the time, a high B12 traces back to something the patient took or was given. A complete exposure history often explains the result before additional evaluation is needed.
Oral supplements, multivitamins, fortified products, and energy products
Oral B12 appears in many products, and much of it is easy to miss on a history. Standalone cobalamin supplements carry the highest doses, often 500 to 1,000 mcg per tablet, while B-complex and multivitamin products contain considerably less. (9) Prenatal vitamins add another routine source.
The harder sources to catch are the ones patients do not think of as supplements. Fortified cereals, nutritional yeast, protein shakes, and functional beverages all contribute B12, and energy or wellness products may contain it at doses far above the daily requirement. A patient who denies taking any vitamins may still be getting a large daily load from an energy drink.
When intake is in play, the relevant details are the form, the dose per serving, how often the patient takes it, how long they have been taking it, and how recently.
Parenteral cobalamin and timing-sensitive interpretation
Injected B12, given intramuscularly or subcutaneously and described as parenteral, is an expected cause of a high serum value. A patient on a loading schedule of frequent injections will show higher levels than one on monthly maintenance, and the timing of the last dose relative to the blood draw can change interpretation.
Elevation after an injection can also linger, partly for a chemical reason. Excess hydroxocobalamin can bind to other plasma proteins such as albumin, which helps explain the very high B12 levels seen after injections of that form. (4) How long the elevation lasts depends on the formulation, the regimen, and the assay, so a fixed clearance time cannot be assumed.
Post-treatment elevation is interpreted differently from elevation without a clear exposure history. A recent injection can account for a high value on its own, and the elevations that merit further attention are the ones with no exposure behind them.
Documenting exposure and interpreting intake-related elevation
A thorough exposure history can resolve many of these cases on its own. It should cover prescription B12, over-the-counter supplements, multivitamins, fortified foods, energy products, and injections, along with the form, dose, frequency, and duration of each. Overlapping products are common, and several modest sources can add up to a large intake.
When intake explains the result and the patient is well, with no concerning clinical or laboratory findings,it can often be attributed as the likely cause without an extensive search for disease. If the picture is still unclear after exposure is accounted for, a repeat measurement after nonessential sources are stopped or timing from the last dose is clarified helps show whether the elevation persists.
Prescribed cobalamin should not be stopped without clinician review, even when a high result prompts the question.
Disease-associated hypercobalaminemia and the differential that changes management
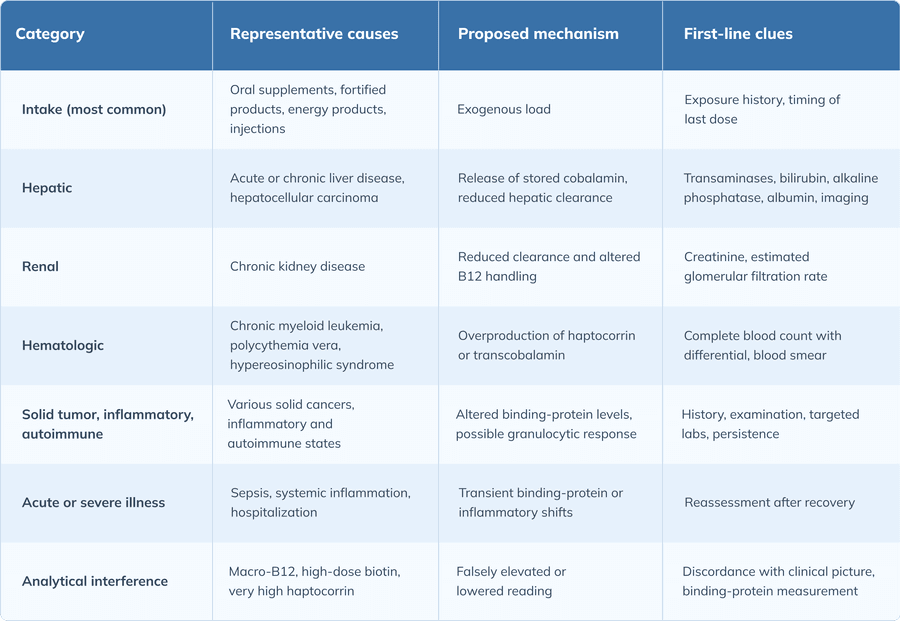
After intake and interference are excluded, persistent elevation can point toward hepatic, renal, hematologic, inflammatory, or malignant disease. The conditions behind it fall into a few categories, and a complete blood count (CBC), liver tests, renal function, and the clinical context often narrow the category.
Hepatic (liver-related) causes
The liver is a major reservoir for cobalamin, so liver disease is one of the more common explanations for a high B12. Hepatocellular injury, meaning damage to liver cells, releases stored vitamin B12 into the blood, and chronic liver disease reduces the clearance that normally keeps levels in check. Elevated B12 is well recognized across liver conditions, including alcohol-associated and other chronic liver disease. (1)
Supporting tests help establish the link to liver disease. Transaminases, bilirubin, alkaline phosphatase, albumin, and markers of synthetic function point toward a hepatic cause when they are abnormal. Hepatocellular carcinoma, a primary liver cancer, should remain on the differential when B12 elevation is marked, persistent, and otherwise unexplained. Both liver cancer and myeloid malignancies have been associated with very high B12. (3)
Renal (kidney-related) causes
Reduced kidney function may contribute to elevated B12 by reducing clearance. Higher B12 has been associated with reduced kidney function in population data, particularly among individuals with higher homocysteine concentrations. (8) Creatinine and the estimated glomerular filtration rate (eGFR) provide the baseline for judging whether kidney disease is contributing to the elevated B12.
Kidney disease becomes a more convincing explanation for a high B12 when renal findings such as an elevated creatinine or a reduced eGFR are present. Without those findings, the elevation is better weighed against the broader metabolic picture and any comorbidities.
Hematologic and myeloproliferative disorders
Several blood disorders drive B12 up by increasing the production of its carrier proteins. Chronic myeloid leukemia, polycythemia vera, and hypereosinophilic syndrome are the classic associations, and the mechanism is thought to be overproduction of haptocorrin or transcobalamin by the expanded cell population. (4)
A CBC with differential is a fast way to triage a hematologic cause. Leukocytosis, thrombocytosis, eosinophilia, anemia, macrocytosis, or an abnormal blood smear all raise the priority of a hematologic cause. Persistent elevation alongside any of those findings is a reasonable trigger for hematology referral. Incident myeloid malignancies are more common in patients whose B12 stays elevated than in those whose levels normalize. (7)
Solid tumors, inflammatory, and autoimmune states
Marked or persistent unexplained elevation has been linked to malignancy in observational data. The proposed mechanisms may involve the same binding proteins, with haptocorrin produced by some tumors and by the granulocytic response, raising the measured B12. (1) Inflammatory and autoimmune conditions have also been reported among associated causes, although the evidence is less consistent than for liver disease, renal disease, myeloid disease, and solid cancer.
These associations are most useful when corroborating findings are present, so the rest of the workup, not the B12 alone, determines how far to go.
Transient elevation in acute or severe illness
Acute infection, a systemic inflammatory state, hospitalization, or other severe illness can push B12 up temporarily. These metabolic shifts are part of why measurements taken during acute illness are interpreted with caution. (6) When the clinical situation allows, repeating the test after the patient has stabilized shows whether the abnormality was passing or persistent.
Elevated B12 and cancer — what the evidence supports and what it does not
A high B12 has been associated with cancer in observational studies, a link that understandably draws attention. The evidence supports a limited association, not broad screening based on B12 alone.
What observational cohorts actually show
Unexplained high B12 has been linked to a later cancer diagnosis, concentrated in the months after the test. In UK primary care, patients with a B12 above 1,000 pmol/L had a one-year cancer incidence rate ratio of 4.72 compared with those in the reference range. (3) Risk in a Danish population was similarly elevated in the year following a high measurement. (2)
The risk is highest in the first year and attenuates afterward, and only a minority of patients with very high B12 were diagnosed with cancer within that year. (3) Persistence adds valuable information. When elevation persisted on a second measurement, the association with incident solid cancer was strong, while a transient elevation carried no greater risk than a normal value. (7)
These are observational cohorts with their own populations, confounders, and limits, so the numbers describe an association in a group, not a prediction for an individual.
Association versus causation
A high B12 can be a marker of possible malignancy, rather than a cause of it. The likely direction is that undiagnosed disease raises B12, not that B12 causes the disease. The risk is highest in the year after measurement, which fits disease that is already present. (2)
Evidence on B12 and cancer is mixed overall, with some studies showing higher risk, some lower, and some none. (9) Most evidence does not support the idea that taking B12 causes cancer, and serum-association studies should not be stretched to say so.
Relative risk and absolute risk look very different. A fourfold or higher relative risk sounds alarming, yet the absolute chance for any one patient stays low.
Translating the signal into proportionate action
Persistent, unexplained elevation can justify further evaluation or a search for occult disease when the history, examination, CBC, liver tests, renal function, or other findings support it.
B12 alone is not enough to justify reflexive imaging, endoscopy, or invasive testing. Because only a small share of patients with high B12 are found to have cancer, the value does not function as a standalone screening test. (3) Checking whether the elevation persists can help identify patients who may need further investigation. (7) A B12 result cannot, on its own, establish or exclude malignancy.
Analytical interference and misleading results
Sometimes the number is misleading, or at least not what it appears to be. A high B12 that does not fit the patient is a reason to ask whether the result reflects an assay artifact.
Macrocobalamin, or macro-B12
Macro-B12, also called macrocobalamin, is B12 bound up in large complexes, most often with antibodies or carrier proteins, that the assay still counts toward the total. Macro-B12 is commonly defined as the fraction of B12 removed by precipitation with polyethylene glycol (PEG). (4) The phenomenon is analogous to macroprolactin, where a large, largely inert complex inflates a routine result.
Well-documented cases exist, but the term is often applied to whatever a nonspecific precipitation step removes, and some studies use methods that cannot actually confirm what was present. (4) Macro-B12 becomes a reasonable consideration when a value is very high, persists over time, comes with no B12 exposure, sits alongside an unrevealing workup, or disagrees with functional markers. A result that does not fit the clinical picture should not be assumed to reflect true hypercobalaminemia, but it should not be assumed to be macro-B12 either.
Immunoassay interference
Other forms of interference can also affect interpretation. High-dose biotin, also known as vitamin B7, can affect assays that use a biotin and streptavidin binding step, and the direction of the error depends on the assay format, with competitive designs prone to falsely high results and sandwich designs to falsely low ones. (5) Routine dietary biotin generally does not reach interfering levels, but high-dose cosmetic or therapeutic supplements can.
Heterophile-antibody interference is less relevant for most total B12 assays. Most total B12 assays capture the vitamin with intrinsic factor rather than an antibody, so these assays are generally not vulnerable to heterophile-antibody interference the way antibody-based assays are. (4) Patterns still vary by platform and vendor, which is why the size and even the direction of any interference cannot be assumed without confirmation from the laboratory that ran the test.
Confirming or excluding interference
Discordance between the result and the clinical picture raises the possibility of assay interference. Re-measuring the sample on a different platform can expose a method-specific artifact. For suspected macro-B12, precipitation with PEG is the test most often reached for, though it is nonspecific and can remove B12 that is fully available to cells, so direct measurement of the binding proteins, haptocorrin and transcobalamin, may be more informative when it is available. (4) Input from the laboratory itself, such as from a clinical pathologist or laboratory-medicine specialist, helps when the result clashes with exposure history, symptoms, and related markers.
High serum B12 with functional deficiency or discordant symptoms
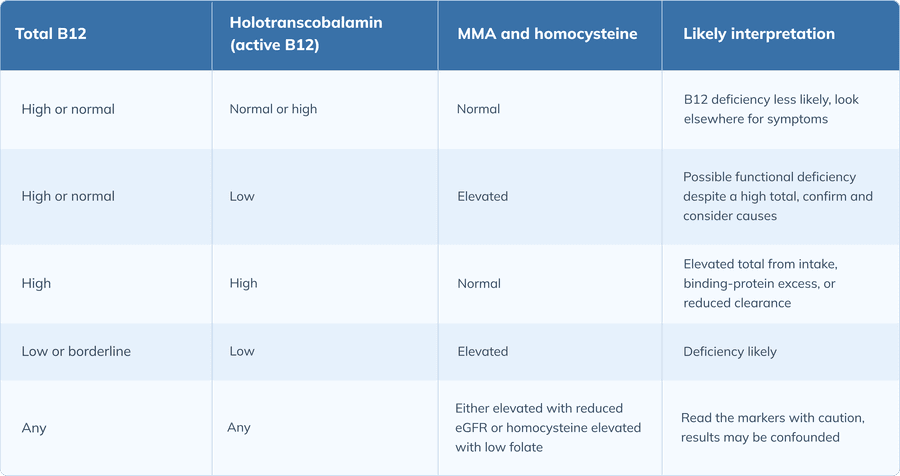
A high total B12 can coexist with a cellular shortage of the vitamin. When symptoms or risk factors suggest deficiency despite a reassuring serum B12 number, functional markers help clarify cellular B12 status.
Why a normal or high total B12 can coexist with cellular deficiency
Total B12 measures what is in the blood, not what has reached the cells, so a high or normal value does not rule out a functional shortfall. A mismatch can develop between the haptocorrin-bound pool, which makes up most of the total, and the smaller active fraction on transcobalamin that cells depend on. Holotranscobalamin and the metabolic markers provide a more informative assessment of functional B12 status than total B12. (6)
Deficiency can be missed in settings such as malabsorption, autoimmune gastritis, certain medication use, and nitrous oxide exposure. In each, B12 status can be impaired even when the total level looks adequate.
Functional and confirmatory markers
Methylmalonic acid (MMA), homocysteine, and holotranscobalamin can provide information that total B12 does not. MMA rises when B12 is functionally lacking inside the cells and is the more specific of the metabolic markers. (6) Homocysteine also rises with low B12, though it is less specific because folate status and kidney function move it as well. (9) Holotranscobalamin, the active fraction, estimates the B12 actually available to cells.
All markers are interpreted against local reference ranges and the individual patient. Reduced kidney function and folate status are major confounders, since both can raise MMA and/or homocysteine independently of B12. (6)
When to pursue functional testing despite a high value
Functional markers are most useful when the clinical picture argues for deficiency even though the total looks fine. Neurologic, cognitive, hematologic, or mucosal features can point to a shortfall, as can risk factors such as malabsorption, autoimmune gastritis, relevant medications, or nitrous oxide exposure. A mismatch between what the patient shows and what the total B12 says is itself a reason to test further. The markers clarify the picture by supporting clinical judgment, not by replacing it.
Non-B12 causes of persistent symptoms with a high result
When symptoms persist and the B12 is high, the symptoms may have nothing to do with B12 at all. Anemia from another cause, thyroid disease, iron deficiency, folate deficiency, inflammatory disease, and metabolic contributors can all produce overlapping complaints, as can medication effects, sleep disorders, and neurologic conditions. A mismatch between the symptoms and the laboratory result is a reason to widen the evaluation.
A practical approach to the unexpectedly elevated result
A practical workup starts with the report, exposure history, prior results, and baseline labs, and moves to repeat testing or referral as the findings warrant.
First-pass interpretation at result review
The first pass stays with the report itself: the numeric value, the unit, the laboratory reference range, and the assay used, since each changes whether the result is even high. Next comes a reconciliation of any supplements, multivitamins, fortified products, energy products, and injections, along with when the patient last took or received B12. Prior B12 values show whether the elevation is persistent or already on its way down, and any CBC, liver tests, or renal function already on file may point to a cause before anything new is ordered.
Structured next steps and repeat testing
Repeating the test is worthwhile when intake, a recent injection, acute illness, or a preanalytical issue, meaning a problem with the sample before it was measured, could explain the value, using the same laboratory or a comparable assay so the trend is interpretable. Targeted evaluation is most appropriate when elevation is unexplained, persistent, or paired with red-flag features, with functional markers added when deficiency remains plausible despite a high total. When the result conflicts with the exposure history, symptoms, and related markers, laboratory-medicine input can help clarify the interpretation.
Escalation and specialty referral
Some findings move the workup beyond primary management. Persistent unexplained elevation alongside an abnormal CBC or differential, constitutional symptoms such as unexplained weight loss, night sweats, or persistent fever, or organ-specific findings all raise the need for referral. The referral destination depends on the accompanying findings: liver findings may point to hepatology or gastroenterology, significant kidney disease to nephrology, abnormal counts or smear findings to hematology, and cancer concern to oncology.
Documentation and communication
Documentation helps the next clinician understand why the result was reviewed, how it was interpreted, and what follow-up was planned. A useful note records the numeric value, the unit, the laboratory range, and the date, along with why the test was ordered and whether the elevation was incidental or clinically prompted. It also captures exposure to supplements, fortified products, energy products, and injections with their timing, the symptoms and examination findings, the comorbidities, and the related laboratory results reviewed, followed by the plan, its rationale, and clear safety-net instructions. The note should also frame the result clearly. A high B12 is not a diagnosis, intake-related elevation is not the same as unexplained persistence, and the cancer association does not establish causation.
Limits of the workup
A B12 value alone neither confirms nor excludes malignancy, and clinical judgment decides whether to observe, repeat, evaluate further, or refer. When a first evaluation is unrevealing but the elevation persists, reassessing at intervals is reasonable. The aim throughout is to avoid both overtesting and premature dismissal.
Causes of elevated serum vitamin B12 by category
Interpreting total B12 alongside functional markers
Frequently asked questions (FAQs)
How should clinicians interpret elevated serum B12 when supplementation or a recent injection is reported?
Reported intake or a recent injection is the likely cause, since oral supplements, fortified products, and injected B12 are the most common reasons for a high value. The form, dose, and timing are worth recording, and further workup becomes necessary if the elevation persists once those sources are accounted for, or if symptoms, examination findings, or other labs raise concern.
When is repeat testing meaningful after oral or parenteral cobalamin exposure?
Repeat testing is informative once the nonessential source has been stopped or enough time has passed for an injection to clear, using the same or a comparable assay so the trend is interpretable. A level that drops back into range supports intake was the cause. If it stays up, the elevation needs a fuller workup.
Which initial laboratory tests best triage an unexplained high B12 before referral?
A complete blood count and differential, liver function tests, and renal function with estimated glomerular filtration rate point toward the hepatic, renal, and hematologic causes that account for most disease-associated elevation. Checking prior B12 values for persistence adds context before any referral.
How should elevated B12 be interpreted in chronic kidney disease or chronic liver disease?
Altered B12 handling and reduced clearance in kidney disease, and both cellular release and reduced clearance in liver disease, can raise B12, so supportive renal or hepatic findings make those causes plausible. A high value should not be attributed to either organ without laboratory or imaging findings that actually support it.
What blood-count patterns should prompt hematology review in a patient with persistent elevated B12?
Leukocytosis, thrombocytosis, eosinophilia, anemia, macrocytosis, or an abnormal blood smear alongside persistent elevation should prompt hematology review. Findings like those suggest a myeloproliferative or other hematologic disorder is producing the excess B12.
When does persistent unexplained elevation justify evaluation for occult malignancy rather than interval observation?
Persistent elevation should prompt an evaluation for occult disease once intake and interference have been excluded, and red flags such as unexplained weight loss or findings specific to organs are present. B12 alone is not a reason to pursue broad imaging or invasive testing absent these supporting signals.
How can clinicians explain the cancer association without overstating risk or implying causation?
A high B12 can mark an undiagnosed cancer rather than cause one, and the likely direction is the illness raising B12. Framing the conversation around absolute risk, which stays low for any individual even when the relative risk looks large, keeps it accurate.
How can macro-B12 be distinguished from true hypercobalaminemia?
Macro-B12 should be suspected when a markedly high value persists with no B12 exposure, sits with an unrevealing workup, and disagrees with functional markers. Confirmation most often relies on nonspecific precipitation, which can give misleading results. Direct measurement of the binding proteins is more informative when available."
How should suspected biotin or heterophile-antibody interference change interpretation of an immunoassay-based B12 result?
High-dose biotin can distort assays that use a biotin and streptavidin step, so holding biotin supplements and re-testing can help when interference is suspected. Heterophile antibodies rarely affect B12 assays, because most capture the vitamin with intrinsic factor instead of an antibody.
When should methylmalonic acid, homocysteine, or holotranscobalamin be ordered despite a high total B12?
These markers are useful when symptoms or risk factors suggest a functional deficiency that a high total B12 could be masking. Methylmalonic acid is generally the more B12-specific marker, while homocysteine and the other markers are best interpreted with kidney function and folate status in mind.
What documentation should accompany follow-up of an incidental elevated B12 result?
Useful documentation includes the value, unit, reference range, date, reason for testing, exposure history with timing, relevant symptoms and findings, and the related labs reviewed. The follow-up plan, with its rationale and safety-net instructions, allows the result to be acted on consistently over time.
The bottom line
A high serum vitamin B12 is usually explained by something the patient took or was given. When intake and interference are accounted for and the elevation persists, the result is interpreted by weighing hepatic, renal, hematologic, malignant, and functional possibilities. The value is a starting point, not a diagnosis, and its meaning depends on the exposure history, the trend over time, the symptoms, and the other laboratory findings around it.
An elevated serum vitamin B12 is best interpreted against the laboratory's own reference ranges and assay context, with attention to the source-sensitive details along the way and escalation to targeted testing or specialty referral reserved for when a clinician-guided pathway supports it.
Sleek consumer lab tests offer data, not direction
Influencer-driven lab companies with AI doctors? That’s not how real health functions. Fullscript Journeys gives you the easy lab testing experience you want and a provider to support you when the real work begins.