Exercise After a Blood Draw: A Clinical Counseling Framework


Patients often ask whether they can train after a blood draw. Consumer health sources tend to answer with confident rules borrowed from blood donation, such as resting for the day or waiting a set number of hours, and those rules may not fit a small diagnostic sample. Venipuncture, the insertion of a needle into a peripheral vein to collect blood for testing, is one of the most common procedures in outpatient care, yet direct guidance on activity timing after a routine diagnostic draw is limited. (10) Much of the advice in circulation is extrapolated from whole-blood donation and therapeutic phlebotomy, where the volume removed and the aftercare expectations are different.
This article offers a risk-stratified framework for advising patients on exercise after a blood draw. It distinguishes the routine diagnostic draw from fasting labs, whole-blood donation, and therapeutic phlebotomy, identifies the patients and circumstances that justify caution, and matches advice to the activity the patient has planned. It stays deliberately bounded, and does not address phlebotomy technique, anticoagulation management, the disease management behind therapeutic phlebotomy, or the workup of syncope. The aim is to let clinicians reassure most patients accurately while recognizing the minority for whom caution or deferral is warranted.
Ready to start delivering better patient care?
Join 125,000 healthcare providers who rely on Fullscript to dispense top-quality supplements and labs to their patients.
Reframing the question: the diagnostic draw among higher-burden collections
Activity advice depends on the patient, the draw, and the planned activity. Separating the routine diagnostic draw from higher-volume collections comes first, because most of the borrowed restrictions originate with those higher-burden procedures.
Physiologic difference between diagnostic venipuncture and whole-blood donation
A routine diagnostic draw and a whole-blood donation both rely on venipuncture, and both are usually taken from the antecubital fossa, the hollow at the front of the elbow. (10) They differ in the volume removed. A diagnostic panel fills a few small collection tubes, while a standard whole-blood donation collects about one pint. (1)
Because a donation removes about that much blood, donor aftercare addresses circulating volume directly. Donor guidance advises against heavy lifting and vigorous exercise for the rest of the day, recommends extra fluids, and tells donors to sit or lie down if they feel lightheaded. (6) The World Health Organization (WHO) frames the same points around preventing bruising at the puncture site and dizziness after the larger collection. (11)
A multi-tube diagnostic sample removes only a small fraction of that volume, so it usually does not create the same circulating-volume concern. Fainting appears less common during outpatient phlebotomy than during blood donation, likely in part because the collected volume is much smaller.
(12) Donation restrictions should not be applied automatically to routine diagnostic draws, because the volume removed and recovery considerations are different.
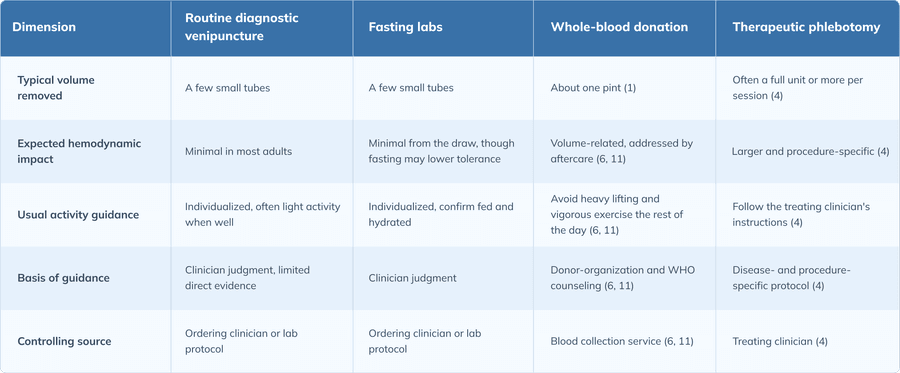
Four collection contexts that change the activity calculus
Four collection contexts commonly prompt activity questions, and they do not carry the same risk. A routine diagnostic draw is a short, small-volume sample, commonly taken from the antecubital veins or, when needed, the dorsal veins of the hand, and it is typically low burden in a well patient. (10) Fasting labs are the same procedure performed after a period without food, so the draw itself is unchanged while the fasting state may lower tolerance in some patients. Whole-blood donation collects a full unit, about one pint, and comes with donor-specific aftercare. (1) Therapeutic phlebotomy, the medically indicated removal of blood to treat conditions such as hemochromatosis or polycythemia vera, is a higher-volume procedure carried out on a schedule set by the treating clinician. (4) These last two are comparison points rather than templates. Conditions such as symptomatic anemia, or an arm with dialysis access, a fistula, or a graft, carry their own restrictions that sit outside routine-draw counseling.
What existing guidance covers and the gap for routine draws
Most written aftercare guidance is donor guidance. Blood collection services advise donors to avoid heavy lifting and vigorous exercise, some for the rest of the day while others such as WHO suggest up to 48 hours, to take extra fluids, to apply pressure and raise the arm if the site bleeds, and to sit or lie down at the first sign of dizziness. (6) WHO gives similar post-donation advice, framed around preventing bruising and dizziness after the larger collection. (11) When applied to a diagnostic draw, this guidance should be recognized as donation-specific, because it was written for a full-unit collection. Direct guidance on exercise timing after low-volume diagnostic venipuncture is limited, so routine-draw advice generally relies on clinician judgment applied to the individual patient rather than on a fixed universal rule.
Reframing the patient question as a risk-stratified decision
A practical way to reframe the patient question is to consider turning a yes-or-no answer into three inputs: the patient, the draw, and the planned activity. Patient factors include antithrombotic therapy, a bleeding disorder, known or suspected anemia, needle anxiety, and a history of fainting with blood draws. Draw characteristics include the site used, whether the draw was straightforward or difficult, whether a hematoma formed, and how much blood was taken. The planned activity ranges from a short walk to a grip-intensive lifting session. These considerations can help inform one of three practical approaches default reassurance for an uncomplicated low-risk situation, targeted caution for an isolated modifier, or deferral when symptoms, higher-volume blood removal, active bleeding, or several flags together raise the stakes.
Venipuncture-site complications exercise can aggravate
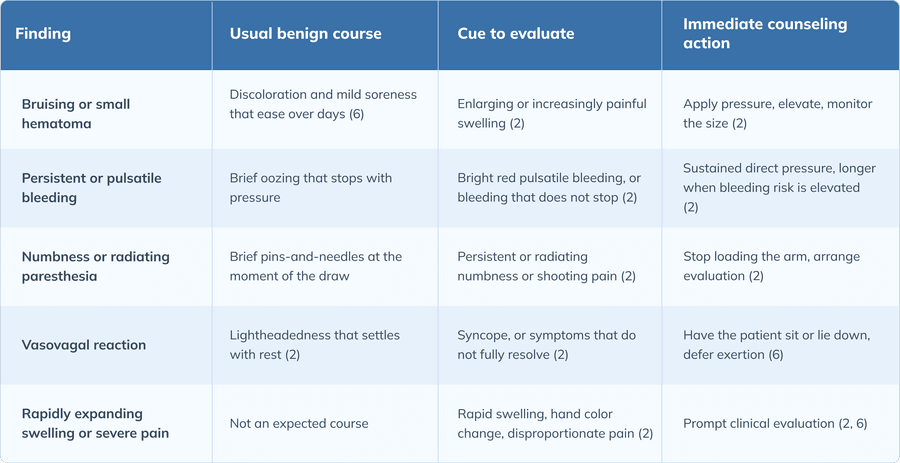
Some post-draw complications are local to the puncture site, and upper-limb exercise can aggravate a few of them. The findings below separate the expected course of a routine draw from the cues that call for evaluation rather than reassurance.
Hematoma, bleeding, and rebleeding at the puncture site
A hematoma is a collection of blood in the tissue around the puncture site, and it forms when blood leaks from a vein that has not fully sealed. (2) Pressure and movement at that site may contribute to rebleeding, so arm-dominant gripping, pressing, and loaded carries on the draw side may be the movements most likely to aggravate it. Confirmed hemostasis, meaning bleeding has stopped and the dressing is intact, is the baseline condition before any exertion. Adequate pressure applied during and after needle removal is what helps prevent hematomas. (2) When bleeding risk is higher, as with anticoagulant therapy or a difficult draw, longer compression and a recheck of the site before the patient leaves may be reasonable.
The antecubital site, elbow flexion, and arm loading
The antecubital site interacts with elbow movement differently than hand and forearm sites. Exercises involving repeated elbow flexion and loading across the elbow joint, such as curls, presses, rows, pulling movements, and grip-intensive work, may apply place mechanical stress on an antecubital puncture, which is why they may be worth a brief pause after a draw at that site. (10) A draw from a dorsal hand vein or the forearm is different, because those sites are generally less affected by elbow flexion, though grip-intensive work can still load a forearm site. Site location is therefore one input into how much arm-specific caution the advice needs.
Nerve irritation and vascular complications requiring evaluation
Most discomfort after a draw is transient. Persistent pins-and-needles, radiating pain, or numbness is different, and it is an escalation cue rather than an exercise-timing question. Nerve irritation has been reported after difficult or repeatedly attempted draw, and it warrants stopping arm loading and arranging evaluation rather than working through it. (2) A small number of findings may suggest a vascular complication such as an arterial puncture and call for prompt attention, including bright red pulsatile bleeding, rapid swelling, a change in hand color, and pain out of proportion to a routine draw. (2) These are recognition cues for the clinician, and they take priority over any conversation about training.
Systemic and patient-level factors that modify timing
Beyond the puncture site, several patient-level factors can affect how soon exertion is reasonable. Each one is a potential systemic modifier, and several can be present in the same patient.
Vasovagal reactions, reaction history, and the recovery window
A vasovagal reaction is a transient autonomic response that can involve an initial increase in heart rate and blood pressure followed by a fall in blood pressure, sometimes accompanied by a slowing of the heart rate, resulting in faintness or a brief loss of consciousness. (2) During or after a draw it typically presents with lightheadedness, pallor, sweating, and nausea, and its likelihood rises with the number of collection tubes drawn and a longer wait beforehand. (12) After a vasovagal episode, exertion and injury-prone activities are best deferred until symptoms have fully resolved, and settings where a recurrent faint could cause harm, such as swimming or solo outdoor running, are worth avoiding for the rest of the day. A history of vasovagal reactions, marked needle anxiety, or a difficult or repeatedly attempted draw shifts counseling toward caution and toward scheduling that allows recovery. (2)
Fasting blood work, hydration, and orthostatic risk
Fasting affects activity tolerance in a way that is separate from the venipuncture itself. Professional laboratory-medicine guidance defines fasting as abstaining from food while water remains permitted, and it recommends that water intake mirror the patient's usual daily volume rather than being withheld. (8) Maintaining hydration is therefore usually appropriate, and it supports both the patient and the draw. Reduced food intake and, in some patients, mild dehydration can lower exercise tolerance and contribute to orthostatic intolerance, the lightheadedness or unsteadiness that can occur on standing when circulating volume is low. (5) Volume depletion combined with strenuous activity may contribute to transient orthostatic hypotension, which is one reason a fasting patient who trains hard may feel faint. (3) Before a fasting patient exercises, it is reasonable to confirm that the fasting requirement is complete, to advise resuming fluids and food when the testing protocol allows, and to check whether the fasting or medication instructions came from a clinician or the test protocol rather than assuming. Fasting alone does not require an activity restriction in a well patient, but combined with intense exertion it can lower tolerance enough to justify individualized advice.
Anticoagulant, antiplatelet, and bleeding-disorder considerations
Anticoagulant therapy, which reduces clot formation, and antiplatelet therapy, which reduces platelet aggregation, can both extend the time a puncture site takes to seal and increase bruising. A known bleeding disorder or coagulopathy lowers the threshold for caution further. In these patients, the site-care points carry more weight: longer direct pressure, attention to the dressing, and clear instructions on the bleeding findings that should prompt a call. (2) The red flags for the patient to watch are the same ones that apply generally, including bleeding that does not stop, spreading swelling, and numbness or tingling. (6) None of this involves changing the medication. Patients should not hold anticoagulant or antiplatelet therapy on their own for routine testing, and any change to a regimen is a decision for the prescribing clinician.
Anemia and the patient who is not "routine"
A label of "routine labs" does not make every patient low risk. In a patient with anemia, exertion can bring on dizziness, weakness, palpitations, or breathlessness, because reduced oxygen-carrying capacity limits exercise tolerance. (9) Known anemia, a low hemoglobin under evaluation, or exertional symptoms during or after the visit all shift the recommendation toward caution or deferral rather than default reassurance. A higher-volume removal in the same patient adds a further reason to hold off on demanding activity until the picture is clearer.
A practical counseling framework for activity after routine venipuncture
The framework below moves from a default position for the straightforward case to the adjustments that specific activities and higher-risk patients require.
Default guidance for the asymptomatic patient after an uncomplicated low-volume draw
For an asymptomatic patient after an uncomplicated low-volume draw, light activity such as walking and gentle movement is generally considered reasonable once hemostasis is confirmed and the patient feels well. Resuming at a lower intensity before returning to more demanding exertion is a sensible default. This default applies only when a short list of conditions is met: bleeding has stopped, there is no lightheadedness, there are no fasting-related symptoms, there is no enlarging bruise, there are no significant arm symptoms, and the draw itself was uncomplicated. (6) If any of those conditions is unmet, the situation moves out of the default and into targeted caution or deferral.
Matching advice to activity type
Activity type changes both the local risk at the site and the systemic demand. Light cardio and gentle movement, such as walking, easy cycling, and mobility work, are generally among the lowest-risk options, with the patient stopping if symptoms appear. Easy running may be reasonable once symptoms are absent and the site is stable, while higher-intensity or longer sessions are better deferred when the patient is dehydrated , or recovering from a vasovagal reaction. Heat, dehydration, and solo outdoor running each warrant additional caution. Resistance training deserves particular attention to the site, because heavy gripping, curls, elbow-flexion presses, rows, and loaded carries on the draw side may be more likely to aggravate an antecubital puncture. (2) A difficult draw, marked soreness, visible bruising, or a larger-volume removal are reasons to add caution or to substitute lower-body or non-arm-loading work. High-intensity and competitive exertion carries the greatest consequences if dizziness, faintness, or unstable hemostasis occurs, so deferring it is generally appropriate when the patient is symptomatic, fasting, hemodynamically unsettled, or anemic, after a donation or therapeutic phlebotomy, or in a safety-sensitive training setting.
Individualizing for higher-risk patients and difficult draws
Risk may be cumulative. Antithrombotic therapy, a difficult draw, a fasting state, and a reaction history each shift counseling on their own, and together they compound. As these factors accumulate, advice moves away from routine-draw reassurance and toward more conservative counseling, similar to that used after large blood volume donation removal. The clinician's task is to place the situation on that scale: reassurance for the uncomplicated low-risk case, targeted caution for an isolated modifier such as a single antecubital hematoma, and deferral when there are symptoms, a higher-volume removal, active bleeding, or several flags at once.
Site-care and red-flag counseling points
Site-care counseling is brief and consistent. It can cover direct pressure, arm elevation when appropriate, dressing retention, dressing replacement if bleeding recurs, resuming normal use of the arm, and avoiding restart of the session if bleeding returns. The red flags that should prompt clinical evaluation include severe or increasing pain, expanding swelling, numbness, persistent paresthesia, a change in hand color, and painful redness. (6) Framing these as counseling points, rather than as a script handed to the patient, keeps the clinician positioned to act on them.
Pre-appointment scheduling, workflow, and documentation
Timing and workflow decisions made before and at the draw can reduce questions that arise afterward.
Coordinating fasting requirements, hydration, and training schedules
Scheduling may reduce conflict between labs and training. Confirming fasting status, timing the draw relative to workouts, and booking routine labs before a rest day or a lighter training day where feasible may help reduce scheduling conflicts. Recent strenuous exercise is also a preanalytic consideration, because it can transiently raise several analytes, including creatine kinase, aspartate aminotransferase, and lactate dehydrogenase, so results in a recently exercised patient may need cautious interpretation. (7) Hydration and recent-exertion context therefore matter for both interpretation and aftercare.
Point-of-draw counseling efficiency and team roles
Brief activity counseling fits naturally into the draw itself. Phlebotomy, nursing, and clinician roles may overlap here, and the trained person performing the draw is often well positioned to confirm hemostasis and provide a brief activity message, escalating to the clinician when a flag appears. Phlebotomy protocols already include screening for a history of fainting and clear procedural steps, which makes this an efficient point to add counseling. (10) Documentation supports continuity: a vasovagal event, a difficult draw, a hematoma or persistent oozing, and the instructions given are all worth recording, in line with institutional policy.
When to advise deferring activity rather than the draw
When a test is clinically needed, the activity is the variable to adjust, not the test. Necessary blood work should not be delayed for a training preference, and the more useful move is to set activity expectations around the draw. Rescheduling considerations do apply in specific situations: a therapeutic phlebotomy or other higher-volume draw close to a competition or a heavy training block may justify individualized rescheduling when clinically permissible. A prior vasovagal or difficult-draw history may also warrant moving the appointment. (4) In most cases, adjusting the activity rather than canceling the test is the more appropriate approach.
Clinical application
A patient on a direct oral anticoagulant had a difficult antecubital draw with a developing hematoma and asked about an arm-focused resistance session that afternoon. Using the framework, identify which flags apply, decide between targeted caution and deferral, and state what to reinforce at the site, without altering anticoagulation.
Three flags apply at once: antithrombotic therapy, a difficult draw, and a developing hematoma at an antecubital site, with the planned session loading the same arm. That combination places the situation past targeted caution and into deferral of the arm-focused session for the rest of the day, because gripping and pressing on the draw side may be more likely to enlarge the hematoma while the site is still sealing. Lower-body or non-arm-loading work is a reasonable substitute if the patient wants to train and feels well. At the site, the points to reinforce are longer direct pressure until bleeding has clearly stopped, keeping the dressing in place, and watching for spreading swelling, numbness, or a change in hand color that would prompt a call. The anticoagulant is not adjusted, and the patient is advised not to hold a dose for the draw.
Frequently asked questions (FAQs)
How should activity advice differ across routine diagnostic draw, fasting labs, whole-blood donation, and therapeutic phlebotomy?
A routine diagnostic draw and fasting labs remove relatively little blood and usually allow individualized light activity when the patient is well, while whole-blood donation and therapeutic phlebotomy may remove a full unit or more and follow donor or procedure-specific restrictions.
Which post-venipuncture symptoms should override an otherwise reasonable activity recommendation?
Dizziness, active or pulsatile bleeding, an expanding bruise, severe pain, spreading swelling, and numbness each override a routine recommendation and call for evaluation rather than reassurance.
When does a difficult or traumatic draw justify deferring upper-limb resistance training?
A difficult draw with marked soreness, a developing hematoma, or continued oozing may justify deferring grip-intensive and arm-loading work on the draw side until the site is stable.
How should advice differ across light cardio, running, arm-dominant resistance work, and high-intensity exertion after the same draw?
Light cardio is usually fine when the patient feels well, easy running is generally reasonable once symptoms are absent and the site is stable, arm-dominant resistance work warrants the most site caution, and high-intensity exertion carries the greatest consequences if faintness or bleeding occurs.
Which patients on antithrombotic therapy warrant extended site precautions before exertion, and what should be reinforced without altering their regimen?
Patients on anticoagulant or antiplatelet therapy, and those with a bleeding disorder, warrant longer compression and a site recheck, with reinforcement of pressure, dressing care, and bleeding red flags, and no self-directed change to the medication.
How should clinicians counsel patients who fasted before a draw and plan high-intensity training the same day?
Confirm the fasting requirement is complete, advise rehydration and resuming intake when the protocol allows, and treat fasting plus intense exertion as a reason to individualize rather than as an automatic restriction.
What post-venipuncture findings should prompt evaluation for nerve injury or vascular complication rather than reassurance about exercise?
Persistent or radiating paresthesia, numbness, and shooting pain suggest nerve involvement, while bright red pulsatile bleeding, rapid swelling, hand color change, and disproportionate pain suggest a vascular complication.
When should known or suspected anemia shift the recommendation toward deferral?
Known anemia, a low hemoglobin under evaluation, or exertional dizziness, palpitations, or breathlessness should shift the recommendation toward deferral, particularly after a higher-volume removal.
How can recent strenuous exercise before a draw affect interpretation of selected laboratory results?
Recent strenuous exercise can transiently raise analytes such as creatine kinase, aspartate aminotransferase, and lactate dehydrogenase, so results drawn soon after hard training may need cautious interpretation.
Who on the care team is best positioned to deliver brief activity counseling at the point of draw, and what should be documented?
The person performing the draw is often well placed to confirm hemostasis and give a short activity message, escalating to the clinician for any flag, and a vasovagal event, difficult draw, hematoma, or persistent oozing along with the instructions given should be documented.
When is it preferable to reschedule the draw, or to adjust the activity rather than the test?
A therapeutic phlebotomy or higher-volume draw near a competition, or a prior vasovagal or difficult-draw history, can justify rescheduling, but a clinically needed test is usually kept while the activity is adjusted instead.
The bottom line
Activity advice after routine venipuncture is a clinical judgment rather than a fixed rule, and it is best individualized to the individual patient, the characteristics of the draw, and the activity planned. Keeping the routine diagnostic draw distinct from fasting labs, whole-blood donation, and therapeutic phlebotomy helps avoid unnecessary restriction in a well patient and missed risk in a patient who needs more caution. For most patients, exercise after a blood draw is generally considered reasonable once hemostasis is confirmed and they feel well, while a minority, identifiable by symptom, patient factor, or higher-volume collection, warrant targeted caution or deferral. A practical next step is to review institutional venipuncture aftercare protocols, confirm source-specific activity and site-care intervals, and align point-of-draw counseling with documented practice.
Ready to start delivering better patient care?
Join 125,000 healthcare providers who rely on Fullscript to dispense top-quality supplements and labs to their patients.