Can Pharmacists Order Labs? Scope, CLIA, and Protocols

A patient walks up to the pharmacy counter, asks for a quick finger-stick test, and waits a few minutes for a result they expect the pharmacist to explain and act on. That single interaction touches several kinds of authority governed by different rules. Whether a pharmacist can order the test, run it onsite, receive and interpret the result, and then adjust therapy depends on separate rules that change with the state, the setting, and the test.
Pharmacist involvement in medication monitoring, point-of-care testing (POCT), and collaborative care has grown across community pharmacies, ambulatory clinics, and health systems. Community pharmacies now hold the second-largest share of CLIA waivers, behind only physician offices. (1) Whether a pharmacist can order labs rarely has a simple yes-or-no answer. Several factors shape it, including state pharmacy and medical practice law, collaborative practice agreements (CPAs), standing orders, statewide protocols, institutional credentialing, payer rules, and the test itself. The Clinical Laboratory Improvement Amendments (CLIA) govern the site that performs the testing, while state law determines who is an authorized person to order tests or receive results. (9)
This article gives your team a framework for deciding when pharmacists can order labs, perform CLIA-waived testing, use results for medication monitoring, and fold pharmacist-led workflows into collaborative care. It treats legal authority, testing-site obligations, interpretation scope, and the authority to act as four separate questions, each governed by different rules.
Key takeaways:
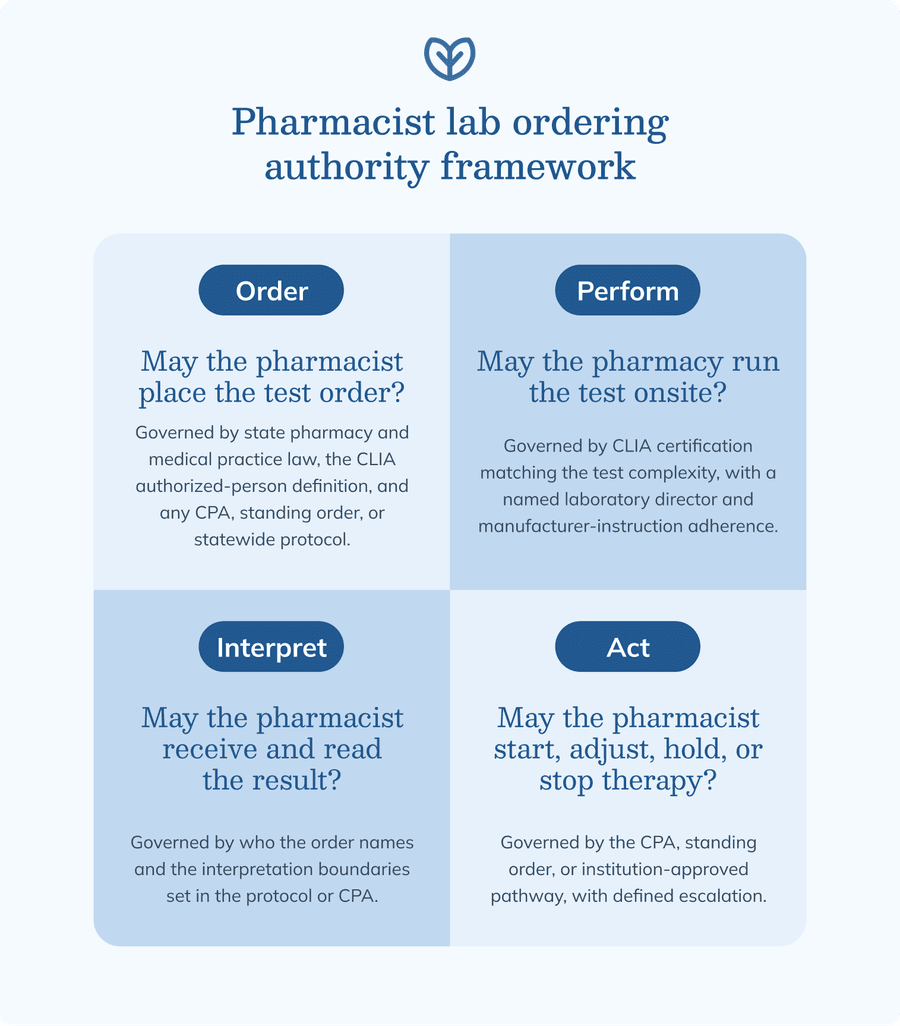
- Pharmacist lab ordering is jurisdiction-, context-, and workflow-dependent, and it separates into four questions: who may order, who may perform the testing onsite, who may interpret the result, and who may act on it.
- Collaborative practice agreements, standing orders, statewide protocols, institutional policies, and CLIA requirements together decide whether a pharmacist-led lab workflow can run safely, and point-of-care testing is never assumed waived without device-specific verification.
- Safe implementation depends on the operational specifics: a defined test menu and result thresholds drawn from guidelines and labeling, reliable routing and escalation for results, and the documentation and quality oversight that keep the program accountable.
Ready to start delivering better patient care?
Join 125,000 healthcare providers who rely on Fullscript to dispense top-quality supplements and labs to their patients.
Pharmacist lab ordering as four distinct authority questions
Pharmacist lab ordering can involve separate authority to order, perform, interpret, and act on results. A pharmacist may be authorized for one step and not another.
Legal authority to order laboratory tests
The legal authority to place a test order comes from state law and may be granted directly, through a CPA, or under a standing order or statewide protocol. Under CLIA, the laboratory must receive a request from an individual authorized under state law to order tests or receive results. (9) Board guidance, payer rules, laboratory acceptance policies, and privileging then decide whether a given order is recognized, and that recognition varies by the specific test and the state.
Operational authority to perform testing at the pharmacy site
CLIA obligations apply to the site that runs the test. Under CLIA, a site becomes a laboratory when it performs even one test on materials from the human body for diagnosis, prevention, treatment, or health assessment, which includes waived tests. (7) A pharmacy that sends specimens to an outside laboratory is the ordering site, while a pharmacy that runs the test at the counter is the testing site and needs its own CLIA certificate, with a named laboratory director even under a Certificate of Waiver.
Professional authority to receive and interpret results
Receiving and interpreting a result are governed by who the order names and the scope the protocol grants. Results may route to the pharmacist, the prescriber, the care team, or a shared record, and CLIA allows release only to authorized persons and those responsible for using the results. (9) Within medication therapy management (MTM), chronic disease management, and test-and-treat protocols, a pharmacist interprets results against defined expected, abnormal, critical, and indeterminate categories. Once the question moves past medication safety into primary diagnosis, a prescriber evaluates it.
Clinical authority to act on laboratory results
Starting, adjusting, holding, or stopping therapy requires explicit authority in the governing agreement or protocol. A pharmacist may take these steps when a collaborative practice agreement delegates that specific function under negotiated conditions, or when a standing order, statewide protocol, or institution-approved pathway authorizes it. (4) The same agreement should name when the pharmacist escalates to a physician, nurse practitioner, physician associate or assistant, or specialist, and should require that decisions and handoffs are documented.
Why pharmacist lab ordering varies by state, setting, and practice model
State scope-of-practice and laboratory law variation
State pharmacy practice acts, medical practice acts, and laboratory laws each define authorized ordering persons differently, and board guidance adds another layer. Uptake reflects this: the share of pharmacies holding a CLIA waiver ranges from roughly 11% to 88% across states, and reporting on which states allow independent pharmacist testing does not always predict actual uptake. (1) Legal authority to order is also distinct from the operational ability to obtain and route results, which depends on laboratory acceptance, payer recognition, and credentialing, so the current rules call for state-specific verification before a protocol is developed.
Collaborative practice agreements and delegated lab authority
A CPA is a formal agreement between a pharmacist and a prescriber that delegates specific patient-care functions under defined conditions. A lab-focused CPA names the covered conditions, eligible patients, and functions the prescriber delegates to the pharmacist, and all 50 states allow pharmacists to enter into one. (4) For medication monitoring, that language sets out which tests are authorized, which medication classes and parameters are in scope, when the pharmacist may adjust therapy, how quickly the prescriber is notified, and how the agreement is reviewed and renewed.
Standing orders, statewide protocols, and institution-specific policies
A CPA delegates authority from a specific prescriber, while a standing order or statewide protocol authorizes a service for a population without an individual prescriber relationship. Public health and test-and-treat protocols are a common example, and pharmacists have dispensed treatment for influenza and group A streptococcus based on test results under such protocols. (11) Health-system protocols and medical staff bylaws shape what a pharmacist may do in a given building, and some states have moved toward a standard-of-care model that authorizes any service consistent with a pharmacist's education, training, and experience rather than itemizing each one. (1) Authority also varies by program type, since pharmacy residency, ambulatory care, and specialty pharmacy services operate under different institutional policies and credentialing.
Payer, laboratory, and EHR constraints
Even with clear legal authority, payers, laboratories, and the electronic health record (EHR) can limit what reaches the patient and the claim. Medicare pays for a diagnostic test that the treating practitioner uses in managing a specific medical problem, and laboratories and payers set their own rules for accepting pharmacist orders. (10) Result routing depends on whether the pharmacist is recognized as an ordering provider, on order-entry permissions, and on the external-laboratory interface, because CLIA limits release to authorized persons and those responsible for using them. (12)
Ordering, performing, interpreting, and acting on lab results
Ordering laboratory tests
Ordering means initiating a test request as an authorized ordering clinician or a delegated protocol participant. The CLIA test request standard expects the laboratory to receive a request identifying the authorized person ordering the test and the tests to be performed. (13) Each order should be tied to a clear purpose, such as monitoring a medication or managing a chronic disease, and Medicare ties payment to a test that informs management of a specific medical problem. (10) The pharmacist who orders the test owns the result and follow-up unless that responsibility is formally handed off, and open-ended diagnostic testing outside the defined scope is left to a prescriber.
Performing point-of-care and CLIA-waived tests
Performing a test onsite means collecting the specimen and running it in the pharmacy or clinic, which is laboratory testing under CLIA. The site needs the certificate matching the test complexity, and a pharmacy performing only waived tests still must hold a CLIA certificate and follow the manufacturer's instructions. (5) Waived test systems are categorized as simple and low-risk when the operator follows the instructions, and the Food and Drug Administration (FDA) categorizes each test by complexity before it reaches the market. (15) Staff training, competency, quality control, and device maintenance keep waived testing reliable.
Interpreting laboratory results within pharmacist scope
Interpretation here centers on medication safety rather than primary diagnosis. A pharmacist reads a result against the patient's baseline, medication history, comorbidities, and concurrent therapies, working inside the categories the protocol defines, and the governing collaborative practice agreement sets the interpretation boundaries and the point of escalation. (4) A result that is discordant, clinically urgent, or pointed toward pathology unrelated to the monitored medication moves to a prescriber for evaluation.
Acting on results under protocolized care
Therapeutic action depends on the agreement or protocol that authorizes it. A pharmacist may adjust a dose for a monitored therapy, or initiate or discontinue a medication, when a CPA, standing order, or institution-approved pathway delegates that decision. (4) Findings outside the protocol move to referral, and critical values or high-risk presentations move to emergency escalation, with the decision rationale and communication pathway recorded.
CLIA requirements for pharmacy-based testing workflows
For pharmacies that perform testing onsite, CLIA status determines the certificate, personnel, quality, and documentation obligations that apply.
When CLIA applies to pharmacy testing
CLIA applies whenever a site tests human specimens for diagnosis, prevention, treatment, or health assessment, which includes pharmacy-based point-of-care testing. A facility is a laboratory under CLIA if it runs even one test on materials from the human body, so ordering a test and performing a test are separate regulatory acts. (7) The certificate category has to match the complexity of the test, because tests are categorized as waived, moderate complexity, or high complexity. (5)
Point of care describes where a test is performed, near the patient, and it is not a complexity category. The Centers for Disease Control and Prevention (CDC) is explicit that a test cannot be assumed waived simply because it is performed at the point of care, since technology now allows more complex testing near the patient. (5) The FDA assigns each test system a complexity of waived, moderate, or high, and a manufacturer must apply for waived status by meeting the CLIA waiver criteria. (15) Before implementation, the exact test system needs verification in the FDA CLIA databases of currently waived test systems, because the certificate type, personnel requirements, and quality systems all follow from that classification. (14)
Certificate of waiver and waived testing responsibilities
A Certificate of Waiver covers simple, low-risk tests and carries a lighter regulatory load than other certificates. A site with a Certificate of Waiver still must follow the manufacturer's instructions and operate good laboratory practices, which means staff know the test system and specimens are handled, timed, stored, and processed correctly. (6) The certificate also names a laboratory director, even though federal CLIA rules set no specific education or experience requirements for a Certificate of Waiver director. (7)
Waiver status applies to a specific test system, manufacturer, and intended use rather than to a general analyte. Each system needs verification against the FDA databases that list currently waived test systems, along with review of the package insert. (14) Treating broad categories such as glycated hemoglobin (A1c), glucose, international normalized ratio, or respiratory testing as automatically waived is a frequent error, because the FDA categorizes by the individual test system, not by the analyte name, and a change in the system, specimen type, or instructions calls for reverification. (15)
Nonwaived testing boundaries in pharmacy-based models
Moderate- and high-complexity testing is nonwaived testing, which most pharmacy point-of-care models are not built to handle. A site needs the matching certificate before performing nonwaived tests, and laboratory-developed tests or tests modified from the manufacturer's instructions default to high complexity. (5) Nonwaived testing brings inspection, proficiency testing, personnel qualification, and quality-system obligations under laboratory director oversight, because the FDA scores each test against defined complexity criteria, so referring it to an external laboratory keeps the pharmacy workflow inside its validated capacity. (15)
Quality practices for pharmacy point-of-care testing
A Certificate of Waiver still needs quality practices that support reliable results. Standard operating procedures, training and competency documentation, and quality control logs record how testing is run, and the CDC offers good-practice resources and a self-assessment for waived testing. (6) Those practices also cover lot numbers, expiration dates, and device maintenance, calibration where the system calls for it, and corrective-action records when a test produces an error or invalid result.
Documentation and result management under CLIA-aware workflows
Documentation ties the order to the result and to the person responsible for acting on it. The CLIA test request standard expects a record of the authorized person, the patient, and the tests requested, and the test report standard governs report content and who may receive it. (13) A complete record captures the order or protocol reference, patient identifiers, specimen details, the performer, the result, and the route, and confirms that results reach authorized persons and those responsible for using them, with retention following institutional and regulatory requirements. (12)
Collaborative practice agreement design for pharmacist lab ordering
A collaborative practice agreement delegates specific lab-related functions from a prescriber to a pharmacist and sets the terms under which tests are ordered, performed, and acted on.
Core CPA elements relevant to laboratory testing
A lab-focused CPA specifies the covered diagnoses or medication-management services, the eligible patients, and the functions the prescriber delegates. (4) It then lists the authorized tests and frequency boundaries, states whether the pharmacist may order, receive, interpret, and act on results, and sets the oversight and escalation model.
Result thresholds and medication-adjustment rules
The agreement groups results into normal, abnormal, critical, and indeterminate categories and ties each to a specific action drawn from current guidelines, drug labeling, or institutional protocol. Dose adjustment, a medication hold, or a therapy change each has a defined trigger, and the agreement names the circumstances that require prescriber approval before the pharmacist acts. (4) The agreement should also state how protocol-concordant actions and discretionary decisions are documented.
Communication and referral requirements
Closed-loop communication assigns responsibility for results that move between the pharmacy and the prescriber. The CPA sets routine notification pathways, abnormal-result escalation timelines, and a critical-result process, and CLIA requires the laboratory to immediately alert the responsible individual when a result is imminently life-threatening or reaches panic or alert values. (12) Handoffs to a physician, nurse practitioner, physician associate or assistant, specialist, or emergency care are documented, with someone named to confirm the message was received and acted on.
Governance, review, and protocol maintenance
Periodic review keeps the agreement aligned with current guidelines, drug labeling, and institutional policy, and the competency of participating pharmacists is reassessed on the same cadence. (4) Governance also covers an audit of order appropriateness, result follow-up, and escalation adherence, with any missed, delayed, or misrouted result reviewed as an incident.
Common clinical scenarios for pharmacist-ordered or pharmacist-used labs
These clinical examples are illustrative, and the specific tests, intervals, and actions in any program come from current guidelines, drug labeling, and the governing protocol.
Anticoagulation management
Pharmacist-managed anticoagulation is one of the most established uses of pharmacist lab work, built around the international normalized ratio (INR). In a family medicine clinic, a pharmacist-managed anticoagulation program kept patients in the therapeutic range more of the time than usual physician care. (18) Under a CPA, the pharmacist adjusts the warfarin dose within defined limits, assesses bleeding risk, and documents dose changes and prescriber communication, with the boundary at the point where an urgent presentation such as active bleeding calls for prompt evaluation by a prescriber or emergency care.
Diabetes and cardiometabolic monitoring
Diabetes and cardiometabolic services lean on A1c, glucose, lipids, and blood pressure to track therapy and risk. With embedded pharmacists working under a CPA, patients with uncontrolled type 2 diabetes were more likely to reach A1c and blood pressure quality targets than those receiving standard care. (17) The pharmacist reviews adherence, monitors therapy, and modifies treatment where the protocol allows, and uncontrolled disease, hypoglycemia risk, or a finding that raises a new diagnostic question is a trigger to refer.
Renal function monitoring for medication safety
Renal monitoring functions as a medication-safety input rather than a diagnostic workup. Serum creatinine, estimated glomerular filtration rate (eGFR), and a basic metabolic panel flag when a renally cleared or high-risk medication needs a different dose, and pharmacist review of renally dosed medications is associated with low rates of dosing errors. (16) Whether the pharmacist adjusts the dose directly or consults the prescriber depends on the protocol, and rapidly worsening kidney function moves quickly to the prescriber.
Hepatic monitoring for potentially hepatotoxic therapy
Liver chemistry review supports the safe use of medications that can affect the liver. In a specialty neurology clinic, adding a pharmacist improved adherence to manufacturer-recommended monitoring, including hepatic function tests for high-risk medications. (8) Baseline and interval monitoring follow the drug labeling and protocol, and the pharmacist holds therapy, notifies the prescriber, or refers when a result crosses the defined threshold or when liver findings are nonspecific.
Infectious disease test-and-treat models
Test-and-treat models pair a CLIA-waived point-of-care test with a protocol-based treatment pathway where state law allows it. Community pharmacies have implemented waived point-of-care testing for influenza with pharmacist-initiated treatment under collaborative arrangements. (11) Point-of-care tests have diagnostic limits, so the protocol should define when a negative test, a complex presentation, or a treatment failure prompts referral, and a pharmacy performing the test still needs a CLIA certificate and adherence to manufacturer instructions. (6) The protocol should also address antimicrobial stewardship, resistance concerns, and any public health reporting duties that apply to the test or condition.
Specialty pharmacy and high-risk medication monitoring
Specialty pharmacy adds laboratory monitoring to adherence and safety surveillance for high-risk medications. A health-system specialty pharmacy model integrates pharmacists into clinics to coordinate medication access, monitoring, and follow-up. (2) Pharmacists working under collaborative drug therapy management (CDTM) agreements have improved adherence to recommended laboratory monitoring for high-risk specialty medications. (8) Specialty medications are managed across specialist clinics, infusion centers, and external reference laboratories, so the relevant results come from separate systems. A pharmacist coordinating that care confirms each result is retrieved and reviewed, and escalates promptly when monitoring reveals treatment-limiting toxicity or required testing is incomplete.
Implementation checklist for provider organizations
Scope and authority verification
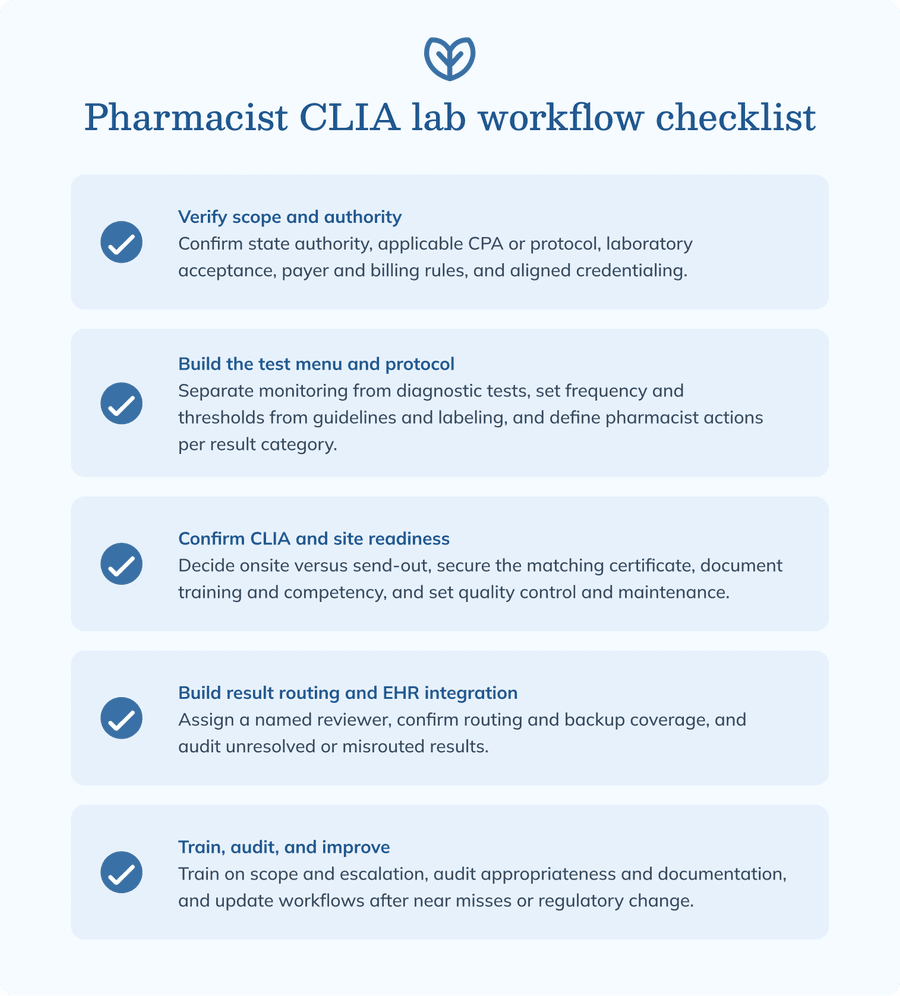
Verify state pharmacist lab-ordering authority and confirm whether a CPA, standing order, statewide protocol, or institutional policy applies, since the authorized-person definition relies on state law to determine who may order tests or receive results. (9) Confirm that the laboratory will accept pharmacist orders, check payer and billing constraints, and align credentialing with the responsibilities you plan to assign, because reported authority and actual uptake do not always match. (1)
Test menu and protocol development
Define the test menu by condition, medication, and workflow. Separate routine monitoring tests from diagnostic workup tests, set frequency and repeat-testing criteria, and specify the result thresholds and pharmacist actions for each category, with the specifics drawn from current guidelines and drug labeling and documented in the CPA. (4) A test-and-treat menu should reflect that the underlying authority is state- and protocol-dependent. (11)
CLIA and testing site readiness
Decide whether testing happens onsite or goes to an external laboratory, because that choice determines the CLIA obligations. Onsite testing means the site is a laboratory and needs the certificate matching the test complexity, even for waived tests. (7) Document staff training and competency, establish quality control and error-management procedures, and treat manufacturer-instruction adherence as a standing workflow requirement, while a send-out model trades onsite obligations for responsibility to track the returning result. (6)
Result routing and EHR integration
Result routing needs explicit ownership because missed or misrouted results may not be obvious right away. Build the order-entry and result-routing pathways, assign a named reviewer for each result, and confirm who owns a pending result from order placement through acknowledgment, because failure to follow up on test results is a recognized and preventable safety gap. (3) Define backup reviewer coverage and confirm whether external laboratories can route results to the pharmacist, prescriber, or a shared pool, because CLIA limits release to authorized persons and those responsible for using the results, so audit unresolved and misrouted results regularly. (12) Documentation templates should capture the pharmacist assessment, action taken, prescriber notification, and audit-trail status so the managing team can confirm the result was reviewed.
Training, audit, and quality improvement
After launch, pharmacist lab programs need training, competency review, documentation audits, and a process for correcting missed or delayed follow-up. Train pharmacists and support staff on the protocol scope and the escalation pathway, and reinforce competency for waived testing using CDC good-practice resources. (6) Audit order appropriateness and documentation completeness, review missed results and communication failures, and track protocol adherence, drawing on the governance built into the CPA for a regular cadence and a place to record changes after adverse events or regulatory updates. (4)
Risk management and referral boundaries
The higher-risk situations in lab monitoring are critical results, delayed or after-hours results, and findings that fall outside the protocol.
Critical results and urgent escalation
Critical values need a predefined handling process and a fast path to the right clinician. CLIA requires the laboratory to immediately alert the responsible individual when a result indicates an imminently life-threatening condition or reaches panic or alert values. (12) That process covers the immediate communication requirements, the emergency referral criteria, the documentation of time-sensitive escalation, and backup coverage for after-hours or delayed results.
Asynchronous, delayed, and after-hours result follow-up
Send-out testing creates a gap between order placement and result review. A send-out workflow needs assigned ownership for pending results, backup coverage for results that return outside pharmacist availability, and a defined pathway for critical results after the pharmacy closes, since failure to follow up on results is a documented source of patient harm. (3) When the pharmacist who ordered the test is not the patient's longitudinal clinician, the workflow names who takes responsibility for an abnormal result. The record captures result acknowledgment, patient contact, prescriber notification, and any unresolved follow-up.
Unexpected abnormal findings and diagnostic uncertainty
Some results fall outside the reason the test was ordered and need a defined referral pathway. An abnormal finding that points to pathology beyond medication monitoring goes to a physician, nurse practitioner, physician associate or assistant, or specialist, and the CPA defines when the pharmacist escalates the result to a prescriber. (4) Stretching the protocol into diagnostic management is the risk to avoid, and handoffs are written in language that preserves both the clinical uncertainty and the urgency.
Symptoms or clinical context outside protocol
A symptomatic patient can exceed what lab-only management can safely handle. Red flags that call for in-person evaluation or emergency care override a protocol built around routine monitoring, and the agreement names the conditions that pause the pharmacist-led workflow. (4) Pregnancy, pediatric patients, and significant renal, hepatic, or immunocompromising conditions act as scope modifiers and are each a reason to transfer responsibility to the managing clinician.
Liability, documentation, and closed-loop follow-up
Documentation shows whether the loop closed, because unaddressed test results are a recurring safety and liability concern. (3) A complete record shows who owned the order and the follow-up, the patient's eligibility for protocolized care, when each result was reviewed and by which clinician, the prescriber notification and acknowledgment, and the routing pathway, since CLIA expects results to reach authorized persons and those responsible for using them. (12) Any misrouted or unaddressed result is reviewed as an incident.
Strategic fit for pharmacist-supported lab ordering programs
Services with structured monitoring, defined protocols, recognized authority, and reliable result routing are better suited to pharmacist lab ordering.
Clinical services most compatible with pharmacist lab workflows
The most compatible services have structured monitoring, defined targets, and an established collaborative relationship. Anticoagulation clinics are a long-standing example, where pharmacist management improves time in the therapeutic range. (18) Diabetes and cardiometabolic management show a similar pattern, with pharmacist collaborative care improving glycemic and blood pressure measures. (17) Medication therapy management, chronic disease co-management, specialty pharmacy monitoring, and authorized public health test-and-treat programs follow the same pattern, each pairing scheduled monitoring with a defined protocol or collaborative relationship.
Situations where pharmacist lab ordering may be poorly suited
Pharmacist lab ordering is harder to support when authority, infrastructure, or accountability is unclear. Unclear legal authority, no shared EHR or reliable result-routing pathway, and an undefined prescriber backup process each undermine a safe workflow, and inadequate CLIA infrastructure is another limit, since onsite testing requires the certificate that matches the test complexity. (5) Diagnostic complexity beyond protocolized medication management, and payer or laboratory refusal to recognize pharmacist orders, also point toward a different pathway, because reported state authority does not guarantee that orders will be accepted in practice. (1)
Interprofessional workflow design
Interprofessional lab workflows need defined responsibilities for pharmacists, physicians, nurse practitioners, physician associates or assistants, nurses, care coordinators, and laboratory personnel. Communication pathways cover both routine and abnormal results, the CPA framework defines shared documentation standards, escalation, and coverage, and feedback loops between the pharmacy and the primary or specialty care teams keep monitoring connected to the rest of the patient's care. (4)
Sustainability of pharmacist-supported lab monitoring
Sustainability depends on maintaining the conditions that made the program safe at launch: a protocol review cadence, compliance monitoring, staff-training updates, reliable result routing, and quality and safety metrics specific to pharmacist-ordered or pharmacist-used labs. The governance written into the CPA gives the program a structure for that ongoing review. (4) Feasibility is reassessed periodically, and the workflow adapts as state law, payer rules, and laboratory policies change, since the legal landscape for pharmacy testing continues to shift. (1)
Frequently asked questions (FAQs)
When can pharmacists order labs independently versus under delegated authority?
A pharmacist may order labs independently only where state law grants that authority directly. In many states, ordering is delegated through a collaborative practice agreement, standing order, or statewide protocol, so the answer depends on the jurisdiction and the test.
Which pharmacist lab-ordering activities usually require a collaborative practice agreement?
Activities that involve ordering tests, interpreting results, and adjusting therapy for a specific prescriber's patients typically run under a collaborative practice agreement.
How should organizations distinguish medication-monitoring labs from diagnostic testing?
Medication-monitoring labs track the safety and effect of a known therapy against defined parameters, while diagnostic testing investigates a new clinical question.
What laboratory result thresholds should trigger prescriber escalation?
Critical values go to the prescriber right away, along with results that land outside the protocol's range or point to a problem unrelated to the monitored medication.
How should pharmacist-ordered results be routed in shared or fragmented EHR environments?
Each result needs a named reviewer and a confirmed route from the laboratory to the pharmacist, prescriber, or shared pool, with backup coverage for delayed or critical values.
What governance safeguards reduce risk in pharmacist-managed anticoagulation monitoring?
Anticoagulation programs lean on a few safeguards: dosing limits the pharmacist stays within, documented patient contact, a defined path for escalating bleeding or out-of-range values, and routine audit of follow-up.
How do CLIA-waived testing obligations affect community pharmacy workflows?
Even one waived test makes a community pharmacy a CLIA laboratory. Day to day, that means training whoever runs the test, keeping quality control current, and following the manufacturer's instructions exactly, all under the pharmacy's Certificate of Waiver.
What should provider teams verify before adding A1c, INR, glucose, or infectious disease testing in pharmacy settings?
Verify each test system's CLIA complexity and waiver status by device, confirm the site holds the matching certificate, and confirm state ordering authority, laboratory acceptance, and payer recognition.
How should abnormal results outside the pharmacist protocol be documented and handed off?
Document the abnormal finding, the time of review, and the responsible clinician, then hand off to a prescriber or specialist in language that preserves the clinical uncertainty and the urgency. Confirm that the receiving clinician acknowledges the result.
What operational barriers commonly prevent pharmacist lab ordering from scaling safely?
Common barriers include unclear legal authority, laboratory or payer non-recognition of pharmacist orders, fragmented result routing, undefined prescriber backup, inadequate CLIA infrastructure for onsite testing, and gaps in competency maintenance.
The bottom line
Pharmacist-supported lab ordering strengthens medication monitoring and collaborative care when its legal authority, CLIA readiness, and accountability are settled up front. A practical first step is to confirm where your state's scope rules, CLIA obligations, institutional policies, and collaborative practice agreements stand before pharmacist-led testing launches or expands. Fullscript can help your practice integrate lab ordering and testing, making it easier to manage multiple orders and labs in one place.
Jurisdiction note: This article focuses on U.S. pharmacy and laboratory workflows. State law, institutional policy, payer rules, and laboratory acceptance policies vary and should be reviewed before implementation.
Ready to start delivering better patient care?
Join 100,000 healthcare providers who rely on Fullscript to dispense top-quality supplements and labs to their patients.