Can Holistic Providers Order Labs? Scope, Law, and Safety

At holistic, functional, and integrative practices, patients often arrive with a specific test in mind, such as a hormone panel they read about or a direct-access test they want to order themselves. The request carries an unspoken assumption that the practice's holistic or functional identity is what lets the provider place the order. Whether that is true depends on the provider's license and state law.
Laboratory ordering is governed by who counts as an authorized person, by state scope-of-practice law, by the ordering individual's license category, and by the laboratory's own acceptance policy. Under the Clinical Laboratory Improvement Amendments (CLIA), a laboratory needs a request from an individual authorized under state law to order tests or receive results. (7) Words like holistic and functional describe a care approach, and the terms complementary, alternative, and integrative refer to how non-mainstream care is combined with conventional medicine. (10)
This article clarifies how you and your team can explain holistic provider lab-ordering authority to patients and to one another. It works through licensure, state law, laboratory policy, direct-access options, insurance implications, and safe follow-up, so the ordering pathway is clear before a specimen is drawn.
Key takeaways:
- Authority to order labs comes from licensure, state scope of practice, the CLIA authorized-person rules, and the laboratory's acceptance policy, and a holistic or functional label does not by itself establish it.
- Direct-access and cash-pay routes can widen access to holistic lab testing, and they do not change who is responsible for test selection, interpretation, and follow-up, nor do they guarantee insurance coverage.
- Abnormal, urgent, or clinically discordant results need a named responsible clinician and a defined escalation pathway set before testing begins.
Ready to start delivering better patient care?
Join 125,000 healthcare providers who rely on Fullscript to dispense top-quality supplements and labs to their patients.
When holistic providers can order labs
Holistic providers can order labs only when a recognized license and the applicable state law give them that authority, and the laboratory agrees to accept the order.
Holistic providers can order labs only when authorized
For a holistic provider, the authority to order a lab comes from the clinician's professional license, the scope of practice the state grants, and the laboratory's policy on whose orders it accepts. Holistic describes a whole-person orientation to care that clinicians of many license types may adopt, and it carries no independent legal meaning for lab ordering. The CLIA definition of an authorized person turns on whether state law authorizes that person to order tests or receive results. (7) Authority to order is also separate from the authority to interpret, diagnose, treat, or receive results, and a provider may hold one without holding the others.
A laboratory test request is a regulated clinical request governed by federal rules. CLIA requires a written or electronic request from an authorized person, and the requisition must capture the ordering provider's identity, the patient's identity, the test requested, specimen details, and any information needed for accurate testing and reporting. (15) The same rule requires a contact who can receive imminently life-threatening, panic, or alert values, which lets the laboratory reach a responsible person fast.
A four-part framework for ordering authority
Four checks determine whether an order is valid and usable: license, state scope, laboratory policy, and the test's clinical purpose. The professional license is the starting point, since it establishes the category of clinician. State scope-of-practice law is the controlling jurisdictional check, because the same license can carry different authority in different states. Laboratory policy is the operational check, since a laboratory sets its own rules about which provider types it accepts and verifies the ordering provider against its authorized-person and requisition requirements. (7) Test type and clinical purpose add further constraints, and laboratory-side governance, including CLIA certification status and laboratory medical director oversight, sits underneath all of it.
Payment should be reviewed separately from ordering authority because a payer may deny a claim even when the provider has authority to order the test. Medicare ties payment to a test that the treating practitioner orders for a specific medical problem and uses in managing the patient, which makes medical necessity, coding, network status, and ordering-provider eligibility the variables that decide coverage. (8) Cash-pay and direct-access routes can give patients another way to obtain testing, but they do not remove the need for appropriate test selection, interpretation, and follow-up. Direct-access testing operates inside the CLIA framework and the state-law definition of who may order. (1)
Key terms that affect lab-ordering claims
The vocabulary patients use rarely maps to a legal category, and the gap creates risk when an abnormal result returns.
Holistic, functional, integrative, complementary, and alternative care
When practices use words like holistic or functional, they are describing a care approach, and the authority to order a test still rests on the provider's license and state scope. Holistic care refers to a whole-person orientation. Functional medicine is a practice model that clinicians of varied license types use, so the label says nothing on its own about whether the practitioner can order a test. The other three terms, integrative, complementary, and alternative care, have settled definitions from the National Center for Complementary and Integrative Health (NCCIH). A non-mainstream approach used together with conventional medicine is complementary, the same approach used in place of conventional medicine is alternative, and integrative care coordinates conventional and complementary approaches around the whole person. (10) None of these terms is a licensure category.
Patients may hear labels like holistic or functional as a sign that the provider can order, interpret, and act on any lab test. If that assumption is wrong, abnormal results may return without a clearly assigned reviewer. Practices can avoid that gap by documenting the actual ordering person, their license, and the person responsible for follow-up. The authorized-person standard exists precisely to tie a test request to a person the state recognizes. (7)
Licensed clinician, licensed complementary provider, and wellness coach
Several credential categories carry different relationships to laboratory access. Medical and advanced practice clinicians, such as physicians, nurse practitioners (NPs), and physician assistants (PAs), order and interpret tests as a routine part of care. Licensed complementary and integrative health professionals, such as naturopathic doctors, chiropractors, and acupuncturists, are credentialed through state licensure and national certification bodies, and the requirements for treating patients vary considerably from state to state. (11) Nutrition professionals practice under variable state and institutional rules, and federal hospital rules let a qualified dietitian or nutrition professional order patient diets when the medical staff authorizes it and state law permits. (6) Non-licensed wellness and health-coaching roles sit outside this clinical-ordering structure entirely.
Diagnosis, treatment, and lab ordering are licensed clinical acts that a state authorizes. Health and wellness coaching is a patient-centered process built on behavior-change support and patient education, and it does not include diagnosing conditions or interpreting laboratory results. (16) When symptoms, abnormal results, or risk factors call for medical evaluation, the patient needs a licensed clinician, and the authorized-person rule defines who that can be. (7)
A provider-type framework for lab ordering

Lab-ordering authority depends on the provider type, the license involved, and the state rules that define that role.
Conventional medical and advanced practice clinicians
Physicians and osteopathic physicians hold broad laboratory ordering authority within their medical license and applicable state law, including when they practice integrative or functional medicine. Medicare reflects this by allowing the treating practitioner to order diagnostic tests used in managing the patient's problem. (8) A physician working outside their own specialty may still need to route complex results to a colleague for interpretation.
For nurse practitioners and physician assistants, also titled physician associates, lab-ordering authority is tied to the state practice act, the collaboration or supervision arrangement, and the practice setting. Medicare extends ordering to nonphysician practitioners to the extent state scope of practice permits, and institutional policy adds a further operational limit on top of state law. (8) Authority that holds in one state may read differently in another, so a national claim about NP or PA independence does not transfer, and each order is worth checking against the relevant jurisdiction.
Delegated, protocol-based, and institutional ordering follows its own rules. Standing orders and protocol-driven testing let a clinical team initiate labs under a defined protocol, and employer or facility policy can expand or restrict what any individual may order. In many arrangements, the supervising or collaborating clinician holds legal accountability for the order, even when someone else enters it into the system. The laboratory needs a request that names an authorized person and captures the ordering provider's identifiers, which is what makes documentation and result routing work. (15)
Licensed complementary and integrative health professionals
Licensed naturopathic doctors (NDs) may have lab-ordering authority that depends on the jurisdiction. For example, Massachusetts guidance states that a licensed naturopathic doctor may perform or order laboratory and procedural tests to reach a diagnosis or follow disease progression. (5) Licensed naturopathic doctors complete accredited doctoral training and a national board examination, while unlicensed naturopaths lack the same state-recognized credentialing pathway. (11) Scope, the specific test type, and the laboratory's acceptance policy remain three separate checks even where the license clearly exists.
Chiropractors have authority to request or use laboratory testing that depends on the state. Across responding jurisdictions in one national survey, blood analysis could be ordered or performed by doctors of chiropractic, with state-specific limits on related procedures, and the overall scope of chiropractic practice showed a high degree of variability. (4) Specimen type, diagnostic purpose, and the boundaries of chiropractic scope can each constrain what a chiropractor may order, and findings that fall outside that scope call for referral to a clinician who can evaluate them.
Acupuncturists and other licensed complementary providers generally hold narrower and more variable diagnostic authority. Licensed acupuncturists are credentialed through state licensure and, in many states, certification by a national board recognized for the profession. (11) State scope, board rules, certification, and private training each carry different weight, and an order based on a training certificate alone can stall at the laboratory when the state-recognized scope does not cover it. Abnormal findings usually call for co-management with or referral to a clinician who can diagnose and treat.
Nutrition, coaching, and wellness roles
A registered dietitian nutritionist (RDN) often has ordering authority that depends on state law, employer protocol, delegation, or integration into a medical team. Federal hospital rules allow a qualified dietitian or nutrition professional to order patient diets when the medical staff grants the privilege and state law permits it. (6) Laboratory ordering for nutrition-related monitoring is a separate question and should be verified against state law, employer policy, delegation terms, and the laboratory's acceptance rules. An RDN's training covers nutrition assessment, with independent medical diagnosis outside that scope. Institutional ordering privileges come through a medical team that grants and oversees them, and a direct-to-consumer arrangement has no clinician attached.
Health coaches and wellness coaches do not typically hold independent diagnostic or lab-ordering authority under applicable state law. Coaching is a behavior-change and education process delivered in an ongoing relationship, and interpreting laboratory results as a basis for diagnosis can cross into unlicensed practice. (16) When labs are clinically relevant to a coaching client, the appropriate routes are referral to an authorized clinician, a direct-access pathway with defined follow-up, or co-management with a licensed provider.
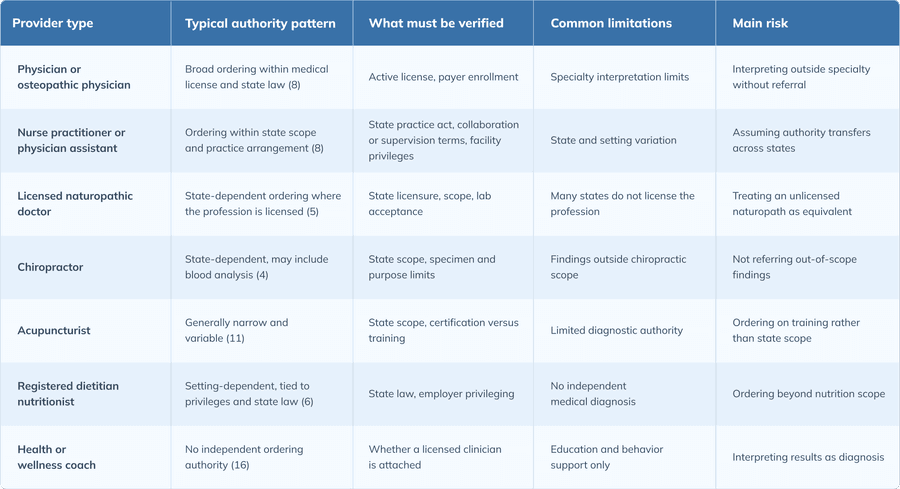
Provider-type comparison
The table below summarizes the typical authority pattern for each provider type, what a practice should verify before relying on an order, the common limitations, and the main clinical or legal risk. Authority varies by state, employer setting, and laboratory policy, so each row is a starting point for verification rather than a national rule.
A verification checklist before holistic lab testing
Before a holistic or functional practice arranges testing, four questions settle whether the order is sound: who is authorized, why the test is being ordered, who owns the result, and how it will be paid for.

Credential and scope verification
Start with the ordering provider's exact professional license and state of licensure, because that pairing sets everything downstream. From there, confirm whether the provider is authorized to order the specific test in the relevant jurisdiction, whether the laboratory accepts orders from that provider type, and whether the provider may receive, review, and act on the results. The CLIA authorized-person standard ties the order to whether state law authorizes the person placing or receiving it, so a verified license in the patient's state is the anchor for the rest of the checklist. (7)
Test selection and clinical rationale
Each test needs a documented reason for being ordered, and that reason shapes how the result will be used. Establish whether the test is conventional, specialty, investigational, wellness-oriented, or supported by clinical guidelines, since the evidence behind it determines how much weight a result can carry. Medicare frames an orderable test as one the treating practitioner uses in managing a specific problem, which is a useful standard even outside Medicare billing. (8) Plan how results will be interpreted. A reference interval is derived from apparently healthy individuals, so an out-of-range value marks a departure to interpret rather than a diagnosis on its own. (14) Define which findings would change management, trigger referral, or require urgent escalation before the test is run.
Result responsibility and critical-value follow-up
Before a specimen is collected, every test needs a named clinician or responsible party assigned to act on the result. The requisition must carry laboratory contact information for imminently life-threatening, panic, or alert values, which is what enables a same-day escalation path for urgent abnormalities. (15) Accreditation standards call for written procedures that define critical results and set who reports them and how fast. (9) Document patient contact attempts and follow-up recommendations, and define the referral or emergency-care route for findings that exceed the ordering provider's scope.
Pricing, insurance, and documentation review
Pricing and coverage should be part of the pre-test review, because patients often assume an order guarantees payment. Distinguish the cash price from the insurance billing pathway, and confirm the medical necessity, coding, network status, and ordering-provider requirements that the Medicare standard ties to payment. (8) For uninsured and self-pay patients, the No Surprises Act requires a provider to give a good faith estimate of expected charges when scheduling a service or on request. (3) Provide a written cost estimate, explain the result-access process, and document the financial conversation so the patient knows what they may owe if a test is not covered.
Direct-access and cash-pay pathways
Direct-access and cash-pay routes widen access to testing, and they raise their own questions about appropriateness, interpretation, and follow-up.
Direct-access testing as an alternative route
Direct-access testing lets a patient initiate testing without a traditional provider order, within limits set by state law and laboratory policy. It operates inside the CLIA framework and the state-law definition of who may order, which differs from provider-ordered testing arranged through a holistic or functional medicine practice. (1) Test menus, specimen collection, result release, and follow-up support vary by laboratory, so the experience is not uniform.
The route fits some situations better than others. Direct access can be a reasonable way to obtain routine or low-risk testing when an authorized provider order is not available. Symptom-driven or high-risk scenarios are a different matter, since they call for clinical assessment that a self-ordered test does not provide. Some direct-to-consumer (DTC) tests may lack the sensitivity and specificity needed for screening and should not stand in for a clinician's evaluation, so abnormal, urgent, or clinically discordant results still need clinician follow-up. (12)
Cash-pay laboratory workflows
In a cash-pay arrangement, the patient pays directly for the test. Direct-access refers to who may initiate or authorize testing, and cash-pay refers to how it is paid for. Under either one, the legal authority to order remains governed by CLIA and state law. (7) Transparent pricing can help patients understand cost, but practices should avoid implying that cash-pay testing is always cheaper, faster, or clinically preferable.
Cash-pay workflows still need safeguards for pricing, result review, and escalation. A clear test menu, published pricing, and a defined result-review process give the patient a predictable experience, and the No Surprises Act sets a baseline expectation that uninsured and self-pay patients receive a good faith estimate. (3) Name a responsible clinician or a defined direct-access follow-up route, and build an escalation protocol for abnormal or critical results before the first specimen is collected.
Functional medicine panels and ordering-authority risks
Functional medicine raises a specific version of the authority question, because the practice model spans clinicians and non-clinicians and often involves broad panels. A panel here is a group of related tests ordered together as a set.
Functional medicine lab ordering follows the ordering person's license
In a functional medicine setting, ordering authority still comes from the individual provider's license, state scope rules, and the laboratory's acceptance policy. A functional medicine physician orders within a medical license, and a functional medicine coach typically holds no independent ordering authority at all, even though both may use the same practice label. A licensed clinician practicing functional medicine can use conventional or specialty laboratories within their scope, and the authorized-person rule still ties the order to a state-recognized license. (7) Scope, medical necessity, and test-type constraints apply the same way they would for any other order, consistent with the Medicare standard that links a test to managing a specific problem. (8)
Conventional tests, specialty panels, and interpretive claims
Standard clinical chemistry, hematology, endocrine, infectious disease, and metabolic tests have well-established reference intervals and clinical uses. Specialty panels are a different category, because guideline incorporation and evidence maturity vary widely, and the clinical utility of certain DTC tests is limited or unproven. (13) A reference interval is defined on apparently healthy individuals and should be distinguished from a clinical decision limit derived from patients with known disease. (14) An "optimal range" promoted by a vendor is neither of those validated benchmarks.
Borderline or unclear results from broad panels still need a defined follow-up plan. Testing a patient with a low pretest probability of disease raises the chance of a false positive, and a reference interval can vary with age, sex, and life stage, so an out-of-range value may reflect physiology rather than disease. (14) False positives, false negatives, incidental findings, and the downstream testing they generate all add burden and risk. Laboratory test overutilization appears most often at initial testing, with roughly one in five tests classified as overutilized across a 15-year meta-analysis. (17) When a broad panel returns a marginal abnormality, the next step may be clinical review before any additional testing is ordered.
When broad panels are tied to cash-pay revenue, the record should show why the tests were ordered and how the results will be used. Many DTC tests are marketed to healthy consumers, with potential harms that include overdiagnosis and the cost of unnecessary testing. (13) Distinguish patient-requested wellness testing from clinically indicated testing, document the clinical rationale whenever a test is ordered or recommended, and keep medical necessity documentation for broad panels, repeat testing, and low-pretest-probability testing, consistent with the standard that ties a test to a specific clinical problem. (8) Claims about diagnosis, prevention, or optimization that the evidence does not support are best left out.
Coverage risk when lab-ordering authority is unclear
For holistic and wellness-oriented tests, assuming that an accepted order will also be covered by insurance can leave patients with an unexpected bill.
Laboratory acceptance does not guarantee payer coverage
Laboratory acceptance means the lab is willing to process the order. Coverage still depends on payer rules, including medical necessity, diagnosis and procedure coding, network status, ordering-provider eligibility, and any prior authorization the plan requires. The Medicare standard frames coverage around a test used in managing the patient's problem. (8) The laboratory's acceptance decision follows CLIA authorized-person and requisition rules, which are different from payment rules. (7) An order can clear the laboratory and still generate a denial when the indication, coding, or enrollment falls short.
Financial risk in wellness-oriented lab panels
Broad wellness panels are a frequent source of non-covered services and patient cost exposure. The cash price, the billed charge, the negotiated rate, the patient's deductible, and any balance-billing exposure can all differ, and a patient who expected coverage may face a bill they did not anticipate. Coverage rules also differ by program, since Medicaid is administered by states within federal requirements, which adds another layer of variation for these patients. (2) Clear pre-test financial disclosure is the safeguard, and for uninsured and self-pay patients the No Surprises Act requires a good faith estimate of expected charges that the practice should document. (3)
Myths, scenarios, and follow-up pathways
A handful of recurring myths contribute to confusion about holistic lab ordering, and a few common scenarios show how the rules play out.
Common myths that create ordering confusion
Myth: any holistic provider can order labs. A holistic approach does not determine legal ordering authority. License, state scope, and laboratory policy do, and the CLIA authorized-person standard ties the order to whether state law authorizes the person placing it. (7) The terms holistic and functional describe an approach to care. (10)
Myth: functional medicine labs always require a doctor. Whether a physician is required depends on the ordering person, the test type, the laboratory's policy, and state law. Provider-ordered, delegated, direct-access, and cash-pay routes are distinct pathways, and direct-access testing operates within CLIA and the state-law definition of who may order without a traditional provider order where the state permits it. (1) The laboratory still needs a request from an authorized person. (15)
Myth: lab acceptance means insurance coverage. Laboratory acceptance and payer reimbursement are separate determinations. Medical necessity, coding, network status, and ordering-provider requirements decide payment, which the Medicare standard ties to a test used in managing a specific problem. (8)
Myth: direct-access labs replace clinical care. Access to a test does not replace diagnosis, risk stratification, or management. DTC results should not be used for diagnosis or treatment decisions or as a substitute for clinical guidance, so abnormal or clinically complex results need qualified follow-up. (12)
Scenario-based ordering pathways
A patient sees an integrative physician or osteopathic physician. This is the standard medical-licensure pathway, and the physician can order conventional and specialty tests within scope. Medicare frames the order around a treating practitioner managing a specific problem, and medical necessity and payer review belong before broad panels. (8)
A patient sees a licensed naturopathic doctor. The pathway depends on the state, since a licensed naturopathic doctor may order laboratory tests to reach a diagnosis where the profession is licensed. (5) Confirm licensure, scope, and laboratory acceptance, and recognize that credentialing and state requirements vary, so findings that exceed scope call for referral or co-management. (11)
A patient sees a health coach or wellness coach. Coaching centers on education and behavior-change support. Medical ordering, diagnosis, and treatment require a licensed clinician with authority under state law. (7) The patient needs an authorized clinician, a direct-access pathway with defined follow-up, or a referral, and a coach interpreting abnormal results risks crossing into unlicensed practice.
A patient wants labs without a provider visit. This is the direct-access and cash-pay pathway, available within CLIA and the state-law definition of who may order, with the test menu and follow-up support varying by laboratory and state. (1) Plan for result follow-up and escalation before testing, so an abnormal value reaches someone who can act on it.
Frequently asked questions (FAQs)
How should clinicians explain lab-ordering authority when patients use the term "holistic doctor" imprecisely?
Explain that holistic describes an approach to care and that authority to order labs comes from the provider's license, state scope of practice, and the laboratory's policy. Ask which licensed professional is actually placing and acting on the order.
Which state-level sources should be checked before stating that a licensed naturopathic doctor can order labs?
Check the state's naturopathic licensing statute, the board or administrative rules that define scope, and the laboratory's acceptance policy for that provider type. Authority exists in some states and not others, so verify the patient's state directly.
When does a wellness provider's discussion of lab results cross into unlicensed diagnosis or treatment?
It may raise unlicensed-practice concerns, depending on applicable state law, when the provider interprets a result as a diagnosis, recommends treatment based on it, or presents an out-of-range value as evidence of disease. Educating a patient about general health concepts stays within a wellness provider's role, and diagnosing or managing a condition is a licensed clinical act.
How should abnormal direct-access lab results be triaged when no ordering clinician is attached?
Route the result to a licensed clinician who can interpret it in clinical context, and treat urgent or critical values as needing same-day attention. An abnormal direct-access result still needs a clinician to interpret it.
What documentation should practices retain when arranging cash-pay or direct-access laboratory testing?
Keep the test menu and pricing, a written good faith estimate for self-pay patients, the clinical rationale where a clinician is involved, and a record of the result-review and follow-up process. This supports both the financial conversation and the duty to act on results.
How should clinicians discuss specialty functional medicine panels with limited guideline support?
State plainly which tests are guideline-supported and which are not, and explain that a vendor's "optimal range" may differ from a validated reference interval or clinical decision limit. Frame results as information that may warrant follow-up rather than a diagnosis.
What payer issues should be reviewed before ordering broad wellness panels through insurance?
Review medical necessity, diagnosis and procedure coding, the ordering provider's eligibility and network status, and any prior authorization the plan requires. Broad wellness panels are often non-covered, which leaves the patient responsible for the charge.
When should a holistic or functional medicine practice refer lab follow-up to primary care or specialty care?
Refer when a result is critical, when it conflicts with the clinical picture, or when interpretation or confirmatory testing falls outside the ordering provider's scope. Set those escalation triggers before testing begins.
The bottom line
Clinically responsible holistic lab testing depends less on the practice label and more on clear authority, appropriate test selection, and reliable follow-up. Before you publish or implement holistic lab-testing guidance, consider reviewing your applicable state scope rules, laboratory requisition policies, payer requirements, and internal follow-up protocols.
Ready to start delivering better patient care?
Join 125,000 healthcare providers who rely on Fullscript to dispense top-quality supplements and labs to their patients.